| Does it Make Sense to Move to a New Location because of Peak Oil? | The Oil Drum: Campfire | Where will our staple foods come from? |
Medical Dark Matter
Posted by nate hagens on February 7, 2010 - 9:10am in The Oil Drum: Campfire
Below the fold is a guest essay from a friend of mine who is an internal medicine M.D. practicing in East-central Minnesota. (He posts on The Oil Drum as 'Rock climber'). The post is a shortened version of a longer essay on the interrelationships between health care, human health, human happiness and resource use. As the healthcare sector makes up fully 17% of the GDP of the USA and therefore represents a significant fraction of our resource throughput, this is a very important topic in discussions of more sustainable systems. If medical care is as inefficient as Rock climber thinks, healthcare policies focusing on basics might save considerable energy and other resources.

Abstract
I’ve been working on problems completely removed from Peak Oil, but the ignorance of big problems and the solutions turned out much the same. “Medical Dark Matter” is my metaphor for ignoring the causes of our relatively poor health.
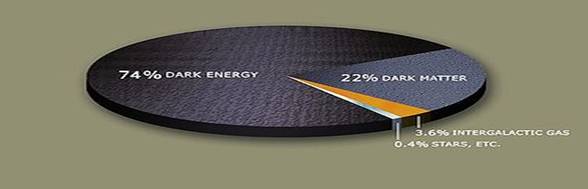
Astronomers looked right past most of reality (96% invisible “dark matter”) until recently. Doctors looked only inside the body and thereby missed about 85% of what really makes people sick or healthy.
Although doctors can save some sick people, they have no power to make most people live longer. Despite over $2 trillion a year of modern medical care, US life expectancy has dropped to 50th in the world (CIA 2009) behind all of Europe and behind some very poor countries. It seems to me that societal factors account for about 85% of differences in life expectancy, with genetics and individual health care accounting for the remainder.
Social factors- differences in our artificially created everyday living conditions- are the real keys to human health. Health is improved by money, social status, healthy early childhood, education and a good job. Poverty and lack of control hurt health. Chronic stress boosts hormones that may harm health. Health choices (diet, exercise, and smoking) are shaped by the neighborhoods we live in, which are influenced by powerful business interests. Income equality is an interesting and controversial factor influencing health. The health of the wealthy may depend in part on the well being of the rest of society.
Money buys health for individual rich Americans, but has failed to make average Americans healthier. What we decide about healthcare reform will have no effect on US life expectancy, since doctors have so little influence on health.
Our American lifestyle takes years off our lives and cannot be sustained indefinitely by available energy resources.
IMPORTANT DISCLAIMER: POPULATION HEALTH IS not individual health I practice conventional medicine; you should keep seeing your doctor.
Introduction: Biology doesn’t determine health
I am an internal medicine doctor and on really good days I save someone’s life. But in the past 20 years I discovered two facts:
1. On the whole medical care has little effect on average lifespan.
2. Social factors can produce 5 year differences in life expectancy.
At first I thought this had nothing to do with Peak Oil. But I realize the different questions have much the same answers. Unless we realign our lives toward healthy sustainability we’ll continue to wreck both our health and the planet. Individuals and societies are largely blind to both our unhealthy lives and our dangerous oil dependence for much the same reasons. We think the status quo is fine and industry “experts” are happy to tell us to keep giving medical and oil corporations trillions of dollars. Like everything else in our artificial modern world, healthcare and energy problems are really economic and social policy issues.
Science is the most powerful way to look at the world. But science once missed the biggest part of reality. In grade school we learned everything in the universe is made of atoms. But in the 20th century astronomers discovered invisible, exotic ‘dark matter’ and ‘dark energy’ actually make up 96% of the universe. (At least science corrects itself; “experts” may not.)
American medicine might be the best in the world. We buy more drugs and spend far more money than anyone else. Then why is our life expectancy (according to CIA statistics) 50th in the world, behind every other industrialized country and some poor ones?
My paper is about life expectancy and population health. Lifespan is more accurate to measure than how well you feel, and usually correlates well with general health. Population studies allow us to figure out average effects (but “your mileage may vary”).
Population statistics explain how I save lives at the hospital, and yet doctors can’t do much for our national health. There are big differences between your individual health and national population health. Consider smoking as an example. If you are really lucky you can smoke cigarettes and still live to be 101. If you get unlucky you might drop dead from a heart attack at age 50. When we look at a large group of smokers, we find smoking takes 5 years (60 months) of life away from the average individual pack a day smoker. Consider a country where 10% of people smoke a pack a day. The national average effect of smoking would be 6 months (10% of 5 years). All these numbers describe smoking risks.
Our very best drugs reduce the fatal heart attack risk in very sick patients from about 6% to 4% over 5 years. That’s a relative 33% less (4/6) or 2% absolutely less (6-4), or a 1 in 50 (100/2% = 50 = number needed to treat to save one) chance of being saved in 5 years, or up to 2 months average life extension. All these different numbers are accepted estimates for our best cholesterol drugs.
Luckily, having a truly life threatening problem is very rare. Most people see doctors for aches or colds, or a chronic problem like cholesterol. Over half my 3000 HMO patients never saw me for years. (Most healthcare is received by “frequent fliers”). Since most people seldom see doctors, the number of lives saved by modern medicine turns out to be far lower than I (and everyone else) once assumed. (Population health is not individual health! If you die it’s tragic, but just a 1 in 300 million statistical fluke).
Medical journals since the 1980’s show that social factors are the real keys to human health. The Whitehall study of British civil servants reported doormen at the bottom died an average 7 ½ years earlier than the bosses at the top. 60% of that gap persists when adjusted for “medical factors”: smoking, obesity, exercise, and blood pressure. More studies followed with similar results.
Social factors produce big differences in life expectancy:
-50 plus year gaps between some poor and rich nations
-4 years gaps between US counties, 6 years between US states
-7 ½ years span from the janitor to the top boss
-6 year gap between high school dropouts and college educated
-5 or 6 year differences between different developed nations
-5 year gap from black race in US, or from male gender
-5 years individual smoking status; few months population average
Medical factors produce very small differences in lifespan:
-Up to 3 month average individual effect of our very best drugs
-few days or no average effect of common preventive healthcare
-I estimate less than 2 months average from all health care effects
The basic circumstances of daily life are the main causes of health and disease.
Is it so surprising people living in tin shack ghettos have different health than inhabitants of Hollywood mansions? Anthropologists know undisturbed hunter gatherers (now extinct) had lifespans in the 70’s. We are genetically identical to our hunter gatherer ancestors, but our cultures (the sum of all beliefs and material goods) are very different. Our genes confirm we are all the same inside but live very differently. Social factors make up our everyday lives: food, shelter and the computer I sit at tonight (and the open sewers of Monrovia’s ghettos).
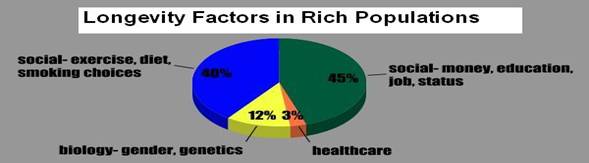
No research is published about how much total medical care affects our lives. I estimate the effect is probably less than 2 months average. If we had no advanced medical care we might live to an average of 78 years instead of 78.1. I estimate 45% social factors (money, education, work and geography), 40% neighborhood shaped choices (exercise, diet and smoking), 12% ‘fixed’ biology (gender and genetics), and no more than 3% healthcare determine average health in rich countries. Society, not biology, underlies 85% of human health. Healthcare may make a 2 month difference, while social factors make 5 year differences in lifespan.
Doctors looked only inside our bodies, when they could have looked outside. “Medical dark matter” points out our blindness:
Only 4% of the universe is made of visible atoms- DARK MATTER is 96% of total reality
Healthcare determines about 3% of longevity in rich countries- Social Factors (MEDICAL DARK MATTER) are 85%
This is dark material. Some doctors have trouble believing what we do is as powerless as I believe. Medical journals present convincing evidence that our profession ignores. It’s hard to admit what we do does so little good. But our tests and medicines might be undone if the patient is poor, stressed out at work, and has no chance to get fresh fruit or walk in fresh air. After hard questioning, I have come to believe the scientific data presented here.
Healthcare’s 2 months is 3 % of the 5 year lifespan gaps from social causes in rich nations.
DISCLAIMER: This paper is not about the overall relative merits of American medicine or of American society. Health is shaped mostly by other factors, irrespective of the inherent quality of medical care. Social factors likely excuse our poor outcomes. America leads the world in individual freedom and prosperity, which may trump years of lost life expectancy.
II. Social Determinants of Health
1. Social Status: Money, Education, Work
-Money (Poverty)
Simple income is the biggest determinant of average life expectancy. Differences between poor and rich countries can be over 50 years and show the importance of basic living conditions to human health.

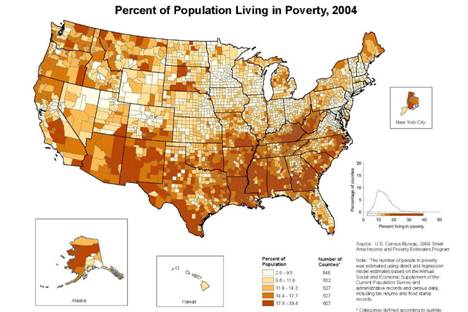
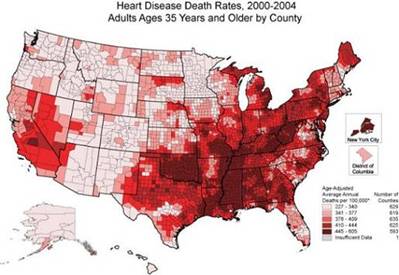
Poverty inside rich countries also harms health. Average people in the worst US county (a South Dakota Indian reservation) die 16 years before those in the longest living county. These maps show poor counties (top) are usually unhealthier (bottom):
-Education
Graduating from college doubles income (to $56,118) and adds 5.9 years to life compared to high school dropouts. Educated people tend to have and make better choices in life. School dropouts are prone to smoking, dead end jobs, and poor health.
Globally, educating girls may save the human race. In the developing world, literate women choose to have far fewer children (the demographic transition). This should continue to slow down the growth of the human population so it doesn’t ruin all planetary resources and wipe out our species in 40 years.
-Work
Workers at the bottom have less control and face more hazards, then get a smaller check, fewer benefits and die 7 years sooner.
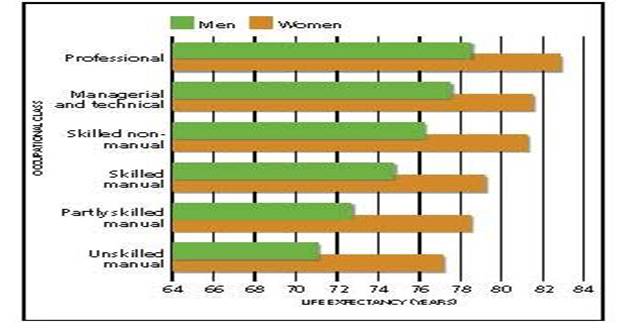
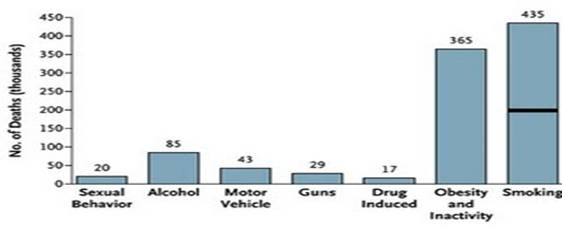
2. Socially Influenced Choices: Smoking, Exercise, Diet
-Recreational Drugs
Smoking is the number one easily preventable cause of death. The poor, uneducated and mentally ill smoke and abuse drugs more. (Rich people drink more alcohol, but more poor people become alcoholic). Doctors’ advice has not been proven to help. Powerful, politically connected businesses heavily promote the use of recreational chemicals, legal and otherwise.
People with rich, fulfilling lives are probably less likely to abuse drugs, analogous to Alexander’s 1970’s animal experiments. A caged rat will repeatedly press a lever for a narcotic high until it starves to death. But if you put a bunch of rats in a big room with interesting toys, they’ll ignore an open bowl of sugar flavored morphine. The #1 prescribed drug in America is now the narcotic pain killer hydrocodone (written 121 million times in 2008).
Opiates are now the opiate of the masses. Are our lives now like lone caged rats?
-Exercise, Diet, Obesity
76% of Americans are overweight or obese. Obesity is painful (arthritis) and shortens life (heart attacks, cancer, diabetes). Obesity cost the US $147 billion in 2008, and diabetes cost $174 billion. As bad as it is, obesity is not the biggest cause of Americans dying too early. Whitehall found job status was more important than obesity and other “medical” factors. Greeks are the second most obese people, but eat healthy food (the Mediterranean diet) and live long lives.
These maps show how much fatter we’ve become state by state in 24 years:



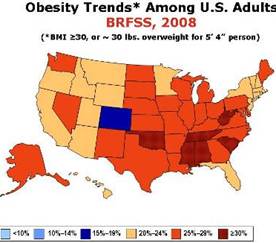
I worked in Africa with people who all wanted to be fat. It looks “rich and comfortable,” but they can’t afford enough food. When I explained that most Americans are fat but wish to be skinny, they asked if Americans have a lack of willpower. It’s not quite that simple. Obesity is a social problem, and especially affects poor and minority people inside rich countries. Powerful government subsidized industries including agribusiness (cheap sugar) and petroleum (cheap gas, compared to elsewhere) influence how easily people can find healthy food or walk in their neighborhoods. See HJ Kunstler’s ‘Big and Blue in the USA’ to laugh and cry.
3. Social/Gene Interaction: Racism, Gender
Gender and race are social definitions. Gender is unique in the oppressed outliving the oppressor (rarely biology trumps society).
Racism is one of our oldest and most emotional social problems. 200 years ago we brought one fifth of our ancestors here as slaves in chains. We put them to work on a continent that was already inhabited. African Americans and Native Americans still don’t get their full shares of the American dream. Race rarely affects health, but racism, poverty and living conditions do.
4. Place, Environment
Our neighborhoods combine other social factors with soil, air and water that might be clean or polluted. 10,000 years ago humans were hunter gatherers living in pristine woods. Then we invented agriculture, towns and cities. Modern poor places have far more physical (lead, cockroaches) and social cigarette billboards) hazards. “Choosing” a healthy life is hard if you live in a city of a million people with bad schools, no jobs (auto industry imploded), and not a single chain supermarket in town since 2007 (Detroit) and all but impossible during two decades of civil war (Liberia, where I worked in 2004).

Consider how differently some peoples live, and how it affects health:

(click for larger image)
III. Income Inequality
“As I’ve often said, this (increasing income inequality) is not the type of thing which a democratic society- a capitalist democratic society- can really accept without addressing”
What flaming liberal is so worried about income inequality?
-Fed Chairman Alan Greenspan, testifying before congress June 2005.
Countries (like Sweden) and US states (like Minnesota) that more evenly divvy up the money tend to be much healthier. Income inequality causes or correlates with many social evils:
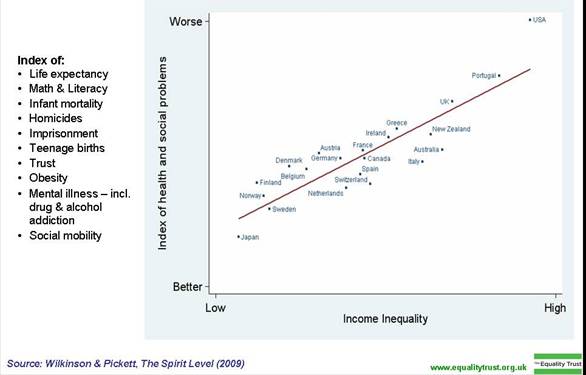
Shorter life expectancy, high infant mortality, obesity, teen pregnancy, mental illness, imprisonment, crime, low educational scores and less social mobility are correlations noted in The Spirit Level published 2009 by Wilkinson and Pickett.
I note apparent correlations with military spending, pharmaceutical advertising and spending, rampant consumerism, corporate power, television watching, low voter turnout, absence of labor unions, automobile use, gun ownership, fast food, sedentary indoor lives, living alone, younger and more mixed populations, and non-denominational religion. A mix of factors including inequality may make some populations dysfunctional. Some societies will decide costs of inequality are worth the gains for those on top.
US inequality worsened in the past 30 years. In 2008 the top 10% of the US population got 48.5% of total income, the top 1% got 23%, and just the top 1/100 of 1% (14,988 families) took 6% of it all.
The authors of the following chart are liberal social scientists, but they might be right about income inequality. I’m uncertain.
Correlation does not equal causation, but there are plausible theories how position in social hierarchy could harm health. The 1.4 billion people living on less than $1.25 daily have trouble getting water, food and shelter. The poor in rich countries are “only” relatively poor. Still the poor, minorities and low level workers have more stress and shorter lives. Stress and feeling lack of control boost neuroendocrine hormones that could shorten life. Sapolsky found wild baboons have graded social stress too. Stress hormones (epinephrine and cortisol) levels fall and lifespans increase step wise up the social ladder to the alpha male, the CEO of baboons. He’s cool as a cucumber, bosses every one else around, and outlives everyone else by years.

IV. The American Paradox: we spend so much for so little
The United States tries to have the best medical care in the world. Yet, in 2009 American life expectancy dropped again to 50th in the world (CIA). We were just surpassed by Wallis and Fatuna (a terribly poor South Pacific territory).
This happened before:
A fable of total 2006 healthcare spending (public plus private):
-Cubans spent $363 per person average (7.1% of GDP); life expectancy was 76 years men and 80 years women.
-Americans spent $6714 per person (15.3% of GDP back then); life expectancy was 75 years men and 80 years women.
-statistics from the World Health Organization 2009.
American healthcare costs $2.1 trillion and one year did not quite match the results of a tiny country that spent only 5% as much per person. This outdated fact is totally anecdotal and totally true.
Almost all other industrialized nations and some poor ones now outlive us. Since rich populations generally do better, this is particularly puzzling. Our lifespan has slowly increased to 78.1 years, but is about 3 or 4 years behind Sweden, Australia and Japan.
The social factors we’ve been discussing plus the fact medical care does not prolong life much on average explains our relatively poor health outcomes. It’s not the fault of doctors. American medical care saves some sick people’s lives, but is just overwhelmed by the negative bigger effects of social problems. The US is very rich, but near the bad end of many other social determinants including income inequality, education (ours kids have lower scores), and jobs (our workers work longer for less benefits). American lifestyle takes years off our lives (and cannot be indefinitely sustained by available energy resources).
V. Conclusion: Healthcare average effects are minimal
Medical Dark Matter is summarized in an outlandish true claim:
Only 4% of the universe is atoms, and healthcare causes only about 3% of health variation- a 2 month difference
Money helps individual rich Americans live longer, but it has not helped our relatively poor national health. We spend $7000 a year per person on healthcare and live no longer for it. Our annual $2.1 trillion dollars is misdirected by believing health is determined inside our bodies. Without modern doctors Americans would probably live to an average 78 years instead of 78.1. How long we live is instead determined by real living conditions: our schools, workplaces, neighborhoods and other social factors.
Disclaimer: My remarks apply only to populations, not to individual health. I share my findings only to help you think about choices our society will make about health and social policy (with or without you).
VI. Consequences
Healthcare’s impotence has consequences for doctors, society and individuals.
The bad health of Americans isn’t doctors' fault. It would be nice to focus on what works best, but retired major journal editors confirm published research has often been skewed by profit interests. Basics like vaccines, sick care and trauma surgery might save more lives than giving more pills to diabetics, but who knows. Good schools and workplaces, and neighborhoods that assist good choices will improve health far more than medical care. It would be cheaper and more effective to treat many diseases as the social problems they really are. Good societal living conditions are the ultimate preventive medicines. Teach girls to read, thus saving the world.
Americans pay to cling to life (average medicare cost $46,412 in the last six months), but we don’t buy anything that might really make us live longer. Why? The medical industry is 17% of GDP and rising. Doctors fail to do basic healthcare analysis and industry supported “experts” gladly fill the gap. Turning over medical care over to corporate interests had the expected results. Deciding whether we want longer lives or bigger profits could be a good start. Unfortunately healthcare reform may happen without any examination of whether medical care works and what it costs.
As a privileged American, I enjoy freedom (I can write this paper) and money. I think everyone should get affordable access to basic healthcare and we should also improve peoples living conditions. Some reasonable people will decide we should continue to maximize individual freedom and material prosperity over other values. The doctor has informed you of benefits and risks. You can decide whether what we get (more money overall) is worth the price (shorter average lives) of American lifestyle and healthcare.
Whatever we decide about healthcare is not very important for lifespan, which is determined by socially created living conditions. Don’t worry (stress is unhealthy). Healthcare reform is an important political and economic issue, but it can’t much affect the health of Americans.
For individuals, the biggest health factor is luck. In the ER I sometimes see a 95 year old man who hasn’t seen any doctor in 30 years, still rides a horse and is healthier than all my other patients. There are no guarantees, but living right (good choices and good neighbors) can improve your odds. Being born to wealth and privilege helps. Working hard for money and an elusive CEO job may be counterproductive. Downsizing your life can be quite satisfying, healthy, and good for the planet. Whether your neighborhood is favorable or not, make yourself exercise a lot (outside if possible) and eat healthy (vegetables, grains, whole foods, not to excess). Working and playing outside with friends deeply satisfies my own hunter gatherer genome.
Please don’t just buy a bunch of guns and hole up. I’m planning on some of you smart TOD people to realign our world financial system so I’ll still have a 401K account in 20 years (and so all the people in Asia don’t live just like us and kill the planet).
Optimists take heart: the global human lifespan probably grew 35 years last century. US life expectancy is also growing slowly, and in 20 years may be where Sweden’s is today (they hit 78 years in 1989). Healthcare does little, but global human living conditions (outside Africa) are improving rapidly, and world population growth is slowing. I believe humans overall will do just fine.

Final Disclaimer: Population Health is not Individual Health. Doctors save the lives of many people every day. I practice conventional medicine; keep seeing your doctor! You can decide if America’s social policies are worth the costs.
Appendix
Ranked Life Expectancy in years, at birth (total both sexes)
Source: 2009 CIA World Fact Book
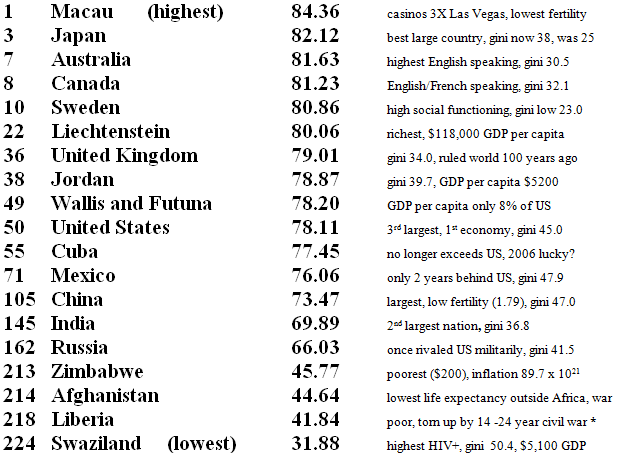
*depends on if you count from Doe (top) killing Tolbert (bottom) in 1980.

Selected Bibliography (over 300 references available)
Adler, N; Stewart, J; et al. Reaching for a healthier life: Facts on socioeconomic status and health in the US. The John D and Catherine T MacArthur Foundation, online at http://www.macses.ucsf.edu/News/Reaching%20for%20a%20Healthier%20Life.pdf
Central Intelligence Agency of the United States Government, CIA World Factbook 2009 data for 224 countries, online at cia.gov/library/publications/the-world-factbook/
Kunstler, James Howard, Big and Blue in the USA. Orion Magazine 2003.online at http://newcities.org/files/iic/BigAndBlue.pdf
Lynch JW, Smith GD, Kaplan, GA, House, JS. Income inequality and mortality: importance to health of individual income, psychosocial environment, or material conditions. BMJ 2000; 320:1200-1204 (24 April)
Marmot, Michael, Social determinants of health inequalities. Lancet 2005; 365: 1099–104.
Marmot, Michael; Wilkinson, Richard; Social determinates of health: the solid facts. 2003 World Health Organization. Regional Office for Europe, WHO Healthy Cities Project, WHO International Centre for Health and Society, online at http://www.euro.who.int/DOCUMENT/E81384.PDF
McGinnis JM, Foege WH. Actual causes of death in the United States. JAMA. 1993;270:2207-2212.
Sapolsky, Robert M, Review: The Influence of Social Hierarchy on Primate Health. Science29 April 2005:Vol. 308. no. 5722, pp. 648 - 652DOI: 10.1126/science.1106477.
Wilkinson, Richard; Pickett, Kate. The Spirit Level: Why Greater Equality Makes Societies Stronger. American version in press, Bloomsbury Press (December 22, 2009)
World Health Organization, Commission on the Social Determinants of Health- final report Closing the gap in a generation: Health equity through action on the social determinants of health 2008 executive summary online at http://whqlibdoc.who.int/hq/2008/WHO_IER_CSDH_08.1_eng.pdf
Contact
- campfire at theoildrum dot com
Personnel
Archives
- November 2010 (4)
- October 2010 (4)
- September 2010 (4)
- August 2010 (6)
- July 2010 (6)
- June 2010 (8)
- May 2010 (9)
- April 2010 (9)
- March 2010 (8)
- February 2010 (8)
- January 2010 (9)
- December 2009 (8)
- November 2009 (7)
- October 2009 (7)
- September 2009 (9)
- August 2009 (9)
- July 2009 (9)
- June 2009 (8)
- May 2009 (9)
- April 2009 (9)
- March 2009 (9)
- February 2009 (9)
- January 2009 (9)
- December 2008 (4)
The Oil Drum: Local archives
- November 2008 (1)
- August 2008 (1)
- July 2008 (4)
- June 2008 (4)
- May 2008 (3)
- April 2008 (1)
- March 2008 (1)
- February 2008 (2)
- January 2008 (2)
- December 2007 (4)
- November 2007 (4)
- October 2007 (6)
The Oil Drum: New York City archives
- September 2007 (3)
- August 2007 (2)
- July 2007 (3)
- June 2007 (8)
- May 2007 (1)
- April 2007 (8)
- March 2007 (2)
- February 2007 (3)
- January 2007 (5)
- December 2006 (5)
- November 2006 (12)
- October 2006 (10)
- September 2006 (9)
- August 2006 (14)
- July 2006 (15)
- June 2006 (11)
- May 2006 (18)
- April 2006 (35)
- March 2006 (14)
- February 2006 (13)
- January 2006 (12)
- December 2005 (17)
- November 2005 (13)
- October 2005 (25)
- September 2005 (36)
License

This work is licensed under a Creative Commons Attribution-Share Alike 3.0 United States License.
wikipedia on smallpox:
"smallpox affected mainly children, with periodic epidemics that killed up to 30% of those infected. "
Such an epidemic would take an average of about 23 years off the life expectancy of the affected population compared to today's values (approximately (75 - 5 (age at death))*0.3 (for the 30%). Therefore, your number for the effects of preventive healthcare is way off: eradicating smallpox through vaccination was an act of preventive health care, your number for preventive health care should be around 30 years, maybe 40 years if you take into account all vaccinations and antibiotics plus isolation of infected individuals. Modern medicine has in fact been extremely successful. It's only that the really successful things are not glamorous: it's not heart transplants that save so many lifes, it's vaccinations, antibiotics and public health reactions to infectious diseases.
Good sanitation and clean water supply also make an enormous contribution (some would argue more than vaccines.)
so does anything that reduces the amount of insulin and igf in the blood stream over time. That is reducing total flour intake, especially bleached white flour. White polished rice, sugar, and other simple carbohydrates.
Fantastic article.
So Bob Marley had it right -- don't worry be happy.
L
A TED Talk on this very subject:
http://www.ted.com/talks/lang/eng/dan_buettner_how_to_live_to_be_100.html
If by some cosmic fluke I were to be appointed US Health Czar, here would be the priorities I would propose to govern our allocation of public expenditure:
1. Relief of pain and suffering. Opiates are a magnificent gift of nature, for which we should be genuinely thankful. They are (or could be) cheap, we are rich. There is no good reason why anyone should suffer agonizing pain when the means is at hand to offer relief. These are dangerous drugs, and a case can be made that access to them must be controlled, but to withhold them from those who genuinely need them in the name of withholding them from those who would abuse them is cruel and barbaric.
2. Prevention and control of infectious diseases. These can sweep through an entire population and cause a massive die-off, and now we have bioterrorism to worry about, so this is actually not just a health care issue but also a homeland security issue. It is absolutely, utterly stupid for people to go around unimmunized because they cannot afford the vaccination. It is also absolutely, utterly stupid to define and defend personal freedom in such an extreme way as to give contgeous people the absolute right to spread infections freely. We don't let people go around spraying machine gun fire at crowds, we shouldn't let infected people spray deadly germs at crowds either. Quarantine is an effective tool, let's use it if needed.
3. Minimize deaths from trauma, by prevention to the extent reasonably possible, and by prompt and effective care for those who are injured. Obviously, if someone is unconscious and bleeding to death you don't want to hold off with treatment until you can find an insurance card - you just get right on it. There is also a homeland security dimension to this: if there is an incident that results in massive casualties, you just need to be prepared to sweep in with as much emergency care as you can muster, do triage, and try to save as many lives as possible.
4. Maximize the productive working lives of children and working-aged adults. This priority is certain to be far more controversial, but it makes sense. An economy needs people who can work productively and contribute to it. Governments need revenue, and they are only going to get it from the economy and the people working it. The more an economy must invest resources in people who are not going to produce a return on that investment through productive working lives, the more of a drag that becomes on the economy. This priority is more difficult to work out, but in general medical interventions that are significantly likely to reduce mortality and morbidity rates in the population below 66 years of age (or whatever the standard retirement rate is) are going to be relevant. So are interventions that will prevent or reduce or minimize disability.
5. Maximize the ability of retirees and the permanently disabled to handle all or as many as possible of the Activities of Daily Living without assistance. It is stupid to deny a knee joint replacement to someone just because they are old and it won't extend their life expectancy, if getting the knee joint replacement will make the difference between their continuing to live independently or having to go into an assisted living center.
These are the only things where I can personally see much of a legitimate and compelling public purpose that justifies the expenditure of much public money. For things that fall outside of these priorities, I'm afraid that an economy that is over indebted and in long-term decline like the US simply can't afford them. If individuals are fortunate enough to have the financial resources to finance such above and beyond care on their own, then more power to them.
I agree that there is a lot of money spent on things that aren't really necessary. Some other thoughts on things that are helpful:
I think safe drinking water is important in maintaining life expectancy. This is not in the current purview of health care, but it needs to be taken care somewhere along the line, or life expectancy will be affected.
Another important issue is safe childbirth. Part of this is having sanitary conditions for giving birth. Part of this is proper nutrition for the mother prior to giving birth. It may be that midwives can handle much of this.
Statistically, men's life expectancy is much better if they are married than if they are single. I think part of this is selection--no woman would marry a man who is clearly has serious problems. Also, men who have serious problems with drugs or alcohol tend not to stay married. And poor people tend to marry less often, so this may also be tied in with the statistical effect. But I think part of this is that if men are in a stable home situation, they tend to do better. They eat better food regularly, and they have something to look forward when they come home from work. So encouraging stable families is probably beneficial (no "marriage tax" for marrying, and no access to welfare benefits because someone is not married).
I am not a life actuary, but from what I remember reading of this issue, it really doesn't extend to women. Single women don't have terribly different life expectancies than those of married women. Of course, if conditions go downhill and strength for outdoor work becomes more important, women might benefit from having a strong helper nearby as well.
Basic sanitation falls under my priority #2, that is all about preventing or reducing contageous diseases. Indeed, it could well be argued that basic public health interventions like clean water and sanitary disposalof human wastes, along with hand washing and sterilization in hospitals, were THE most significant factors in the reduction of mortality and morbidity rates and lengthening of average life expectancies. It should be a very high priority to keep these things running, even if we can no longer afford to give many people many pills.
As for safe childbirth, you are right to point out that mortality amongst women from childbirth used to be frightfully high. Again, simple practices like hand washing and sterilization do help a lot. I am no expert in this area, so I could be wrong, but I suspect that the fact that we now do have the capability to do a C-section in life-threatening deliveries without killing the mother makes a very big difference. This is one thing that should give us a little pause about the otherwise sound idea of relying on midwives. If a delivery does go wrong, it might be necessary to get the mother to the hospital very quickly, and that might not happen in time with home deliveries. If the midwife attended a delivery in a special house that was set up right next door to a hospital (so that the mother could be put on a gurney and wheeled over to the hospital in a couple of minutes), I'd think that would be a much safer plan. As for pre-natal care and maternal nutrition, etc., those do help, but actually have a lot more to do with producing well babies, which fits in my #4 priority; some interventions are thus worth doing, as long as they are evidenced-based and have a strong likelihood of making a significant difference.
Unfortunately, once you venture into such things as marriage - and thus inevitably into such things as how to get people together and how to keep them together (without killing each other) - you really have wandered into the quicksand, if not a minefield. I think the best principle here is the old one: "First, do no harm". Our tax policies, and anything else government does which actually might impact upon marriage patterns in a significant way, should be marriage-neutral. Beyond that, I really doubt that the government can do much that would actually make a positive difference, and am very uncomfortable about the government intruding into people's personal lives to that extent.
Hi Gail and WNC,
re: Gail's comment,
"So encouraging stable families is probably beneficial (no "marriage tax" for marrying, and no access to welfare benefits because someone is not married)."
Gail, did WNC and I both understand you to mean that you support a policy that denies welfare benefits to the unmarried - in general?
Or, do you mean to talk about a female (not a male?) with one or more children?
AFAIK, "welfare", AKA "General relief" (in my State, CA) is for unemployed adults and the income cut-off amount is 300/month. This is 3,600 per year. This is way below the poverty line in CA.
Do you mean that you wish to extend no "welfare benefits" to a female with a child who is not married? (In which case, my first question is: And about the father of the child? Or, if father of child unknown?)
"General relief" comes with a work requirement.
There are many people who simply cannot function in the ways that society demands, in order to secure their basic needs. Such a person may be mentally or physically ill, have substance addiction, temporarily or permanently unemployed or unemployable, or otherwise not able to secure food and housing. And have no other options.
I personally know of two cases (of homeless adults) where the original problem was the apparently "stable" family of the individual in question.
Families can be stable on the surface, in terms of, say, mother and father married, and yet severe physical, emotional or other types of abuse still occur and be perpetrated by the parents.
So, it's not altogether entirely so easy to predict, despite patterns that lend themselves to generalizations.
There are programs other than "General relief" for mothers and fathers of children. (Nutrition program for mothers and infants, etc.) I'm not familiar with all of them.
Do you think people should be denied "charity", as well?
Anyway, in terms of marriage and the culture - it seems what you call "unstable families" really has very little to do with government policies such as welfare, and more, perhaps, in ways related to things like media policies (centralization, conglomeration and
"corporatization" of media), agriculture and transportation policies, labor laws, trade and commerce,etc., i.e., things which, in the surface, may seem unconnected, but which affect the social factors the lead article discusses.
Thanks Aniya.
I think the research suggests that good marriages result in (and result from) better health, diet and income. Bad marriage, on the other hand, results in increased cardiovascular risk factors.
Perhaps the high divorce rate is protective! Think of the health care costs without it! Or maybe divorced people fare even worse than the never-married?
Whatever the case, trying to tweak people's marriage behavior by offering or withholding financial incentives would seem to increase bad marriages, not to improve the quality of existing marriages. So its effect on health could be to worsen it.
It's come to my attention recently that people with ADHD have higher divorce rates. I am developing this understanding of humans as being on a number of scales that determine what environment best suits them. Marriage is an interesting kettle of fish - not for everyone.
1. Opiate addiction is a tricky subject. Administering opiates only leads you to the "law of diminishing returns" by the nature of how opiates work on our brain.
Sorry, I disagree vehemently to your one specific idea of "letting opiates float freely and legally to 'those who deserve it'".
2. Germ control is easier said than done. I don't see any "plan" being proposed by you here. Though I do agree that it is important if we "want to save every human being".
However barbaric that might sound, I'm of the belief that its important to go with the flow, in sync with nature and not try to "fight germs" (quarantine, germ control and thereby "saving populations") or "manipulate nature" (ex: opiate administration). Because, the more we try, the more will nature fight back!
Happiness has nothing to do with long term life expectancy. In this moment of being alive, I'd rather be happy and die the next moment than live a life of suffering (in the "health care bed" or of addiction or of an injury to myself due to a life style that causes harms)
sunson:
As to your #1, that is true, but in terminal patients their life is diminishing faster than the diminishing return on the drug's effectiveness. That's why there shouldn't be a worry about their becoming addicted, either; once they are dead, it won't matter.
I suspect you would feel a little differently about the issue if it were you or a loved one who was suffering in agony and were told that opiates must be denied because of some drug abuse policy.
2. A plan for contageon prevention/control? First, do the things that have made the most difference: basic public health practices to provide people with clean water and the sanitary handling of human wastes. Promote frequent and thorough hand washing, especially amongst health care and food service workers. Sterilize medical equipment and supplies.
Next, do whatever it takes to get the entire population vaccinated against whatever infectious diseases we have vaccines for, and prioritize research funds to develop more of them.
Finally, develop a dense and widespread network of paramedics, nurses and nurse practitioners, and physician assistants, placed and functioning in the neighborhoods and workplaces. One of their primary missions is to be in close contact with the people under their care in order to monitor their health and serve as an "early warning" system for contageon outbreaks. People who come down with infectious diseases need to be treated and isolated promptly. I would propose being much more draconian than we are now when it comes to placing infected people under quarantine.
You are entitled to your view wrt "letting nature take its course", but it would seem to me that if taken to its logical conclusion, it would imply that we should have no medical interventions at all. Indeed, even trying to provide people with clean water and sanitary sewers is the wrong thing to do, because that also goes against nature. If "happiness" is your primary value, then I suspect that most people would be happier if we as a society did what we reasonably could do to relieve pain and suffering and promote health.
I may live longer than the doorman but I have had four diseases that would have killed me:
Gangrene -- thanks to antibiotics and surgery
Melanoma -- thanks to screening and surgery
Colon Cancer -- thanks to screening and surgery
Diabetes -- Gone due to diet and exercise
So, like sanitation, there are factors that extended my life.
Could we do better with a more cost effective system -- yes.
I wonder if the shocking stat about the dramatic decline in money going to doctors was reversed would we all benefit?
Those appear to be a paraphrase instead of a direct quote. It makes for confusing reading when the alleged quote is a couple of pages back.
You are sounding pretty barbaric and thoughtless.
So let me guess, if your child or family member was sick with an infection (malaria, typhoid, cholera, etc.) you would not take them to the doctor and just let nature take its course? What if they recover from malaria without drugs but the parasite damages their liver? Many infections if not controlled can cause permanent damage. It is not just a question of whether you live or die. Many infections (e.g. filaria) if not treated in a timely manner can cause lifelong disability.
Suyog
Great analysis. Just the facts. 17% of GDP {$2.1 trillion} for 2 months additional living based on population data. We in this Country always think we are smart. But in the universe, this has to be one of the worst bargains ever, on a population data basis, of course.
Agreed, especially when so many who are capable of productive lives live with disabling conditions that with care(though currently cost prohibitive) could contribute much to society. Dental care for kids is a fine example. Many many go completely without.
RC:
From Nate's introduction,
"As the healthcare sector makes up fully 17% of the GDP of the USA"
My impression is that we have a trickle down system in "the healthcare sector" in USA.
The health "insurance" sector collects money and passes on to the healthcare delivery
sector only a portion of what it collects. Somewhere in your many references there
must be data that would allow one to determine what fraction of GDP is retained by
health insurance sector. Do you know that number? How much?
Also, it is often claimed that medical malpractice insurance and malpractice tort, and
physician ordering of 'unnecessary' tests to protect against malpractice tort are major
costs. Is this supported, or not, by what you have seen of the data?
As you can easily see, I incline toward trying to find some evil people whom I can blame
for our situation. But your presentation points to environmental problems as a likely
cause of our poor life expectancy. Would you support pulling money out of healthcare
and putting it into environmental remediation? I think I would support pulling money out
of health insurance and putting it into some better delivery channel.
Yes, we have a problem.
So much to say...
First of all, I myself am (was?) an internist, graduated from an elite US medical school. I also have been an member of the academy of anti-aging (or ageing for writers of international English) medicine for several years. However, as longtime posters know, I bugged out to a small remote nation a few years ago. I practiced full time as GP for a couple of years. Now I work part time as the mood strikes and try to enjoy whatever years of BAU might remain.
Pretty much agree with all of the above paper. The truth has always been out there, and my medical school professors taught me the same.
High incomes allow better sanitation and vaccinations. However they also mean unlimited access to cheap unhealthy foods, advertising of the same, and the ability to earn a living without any physical labor. So less infectious diseases, but more obesity and diabetes. So gastric bypass surgery gets added to the GDP, but longevity is a zero sum game.
Now thank goodness for the (relative) anonymity of the internet ...
The details are much too involved to go into online, but to some extent the genetic mechanisms controlling the caloric restriction longevity pathway are being puzzled out. Some people already are taking sirtuin activators, and TOR agents are in the pipeline. If BAU were to continue, it is quite reasonable to expect that many well informed affluent middle aged people alive today could live to be around 120.
Ah, but how much happiness can be obtained by extended health and longevity in a declining world? There's the rub.
Personally, I am childless and in my mid 50s, but appear to be in my 30s. I earned an age group world title in an Olympic sport a few years ago and am now taking up another Olympic sport as a challenge. My parents are both still living approaching 90. One of my ancestors lived to be 97 in the era before electricity without any modern medical care. Minus misadventure, I could expect to live to 2050 in good form, even without considering any theoretical benefit from anti-aging agents. But in the world TOD readers expect, why should I want to?
Conclusion, collapse is here already. Both economic and environmental. The first half of this decade will see Great Depression levels of economic decline (pretty much already here). The second half of this decade will be worse. Most of the shallow water coral in the Caribbean died in 2005 due to the hot water. Ocean acidification with kill the Great Barrier Reef by 2050. Why should one wish to outlive the oceans?
Personally, I have decided to party like it is 1999. In the past few months, I have fully embraced hedonism as the personal solution. Why not? As long as I am having fun with family and friends, I will go on. But I see no reason to continue indefinitely when living conditions become unacceptable. Then it will be time for pills and leaving a good looking corpse.
I find the 20th century focus on general population health as a desirable goal to be ironic. All of the problems facing the world are exacerbated by overpopulation. Even the economic crisis is made worse by the need to support the long lived unemployed, disabled, prisoners, and pensioners. Declining fertility, increased infant mortality, and shorter lifespans are not problems. They are solutions. In fact they are the only solutions humanity is willing to adopt.
The Russian experience post the 1991 collapse is instructive. They turned to alcohol, violent crime, and abortion and are decreasing their population as their resources dwindle. The entire world can and will do the same. We might wish that our loved ones enjoy health and longevity, but should not wish for strangers (competitors for scarce resources) to similarly succeed.
Perhaps post collapse, the world's average life expectancy will drop below 40 again. That would be TEOTWAWKI, but not the end of the world. Da Vinci, Shakespeare, Mozart, and Newton lived in such an environment. Love and life will go on. In the meantime, the whole idea of public health as a social goal will become antiquated.
Very well put. I agree :)
Well ... up to a point.
They actually turned initially, especially the middle-aged men, to heart attacks.
A lot of those primed arteries went pop.
This was not due to famine, nor likely, much, to a sudden increase in alcohol.
Most of the population, and infrastructure, was surprisingly resilient.
BTW. Very effective Guest Post that we are responding to.
Science and epidemiology can really help. At least help define a rational framework.
Phil
That's really grim.
Seems like at age 50+ one might celebrate one's good health and good fortune by devoting the rest of one's life to doing something useful to stop the foolishness that is destroying the planet. It isn't very helpful to run away to remote areas or become obsessed with personal life extension -- and the only possible counter to corporate propaganda is smart, fearless people out on the streets, raising their voices and waving their arms.
The corporate interests are so afraid of public demonstrations they do everything they can to suppress them -- never think that what you believe and say doesn't matter!
And if everyone adopted Rock Climber's implied program (simplicity, personal responsibility and civility) there would be few of the problems that Mike Davis so eloquently describes (Planet of Slums), and at least the forests and the salmon would come back -- whether the oceans would cool off and the coral regenerate, I couldn't say.
My information is about a decade old but may still be valid. In Denmark they have neighborhood paramedics/nurses who you see before going to the doctor. This eliminates a lot of unnecessary visits to the doctor and gives doctors more time to serve those who need them the most.
Somehow we let nurses do triage in an expensive emergency ward but won't let them come to our homes and do the same thing.
What we have in America are paramedics and nurses afraid to say you don't need a doctor and tell you to just stay home and rest until you fell better. We also have doctors afraid not to pursue the most aggressive treatments for people very likely to die from cancer or heart disease within the next year. We have doctors like those my 89 year old step father saw last year who urged him to get a cornea transplant because his insurance and medicare would cover all the cost. We need to get rid of fee for service payments for our doctors and just give them a decent salary and a cadre of nurses and paramedics to call first.
I am amazed at the incredibly expensive surgeries and cancer treatments routinely advised, even when they offer only a 20 - 30% chance of success. In treating the reappearance of her cancer, after chemotherapy didn't work, my mother-in-law's doctors encouraged her to undergo a series of very invasive, expensive surgeries that made the last six months of her life miserable. The surgeries ended up extending her lifespan perhaps a month. Doctors seem to believe that everything that can be done, must be done, regardless of expense, likelihood of success, quality of life or basic reasonableness.
When the doctors told us my that all my mother-in-law's internal organs were shutting down, the next question was whether we wanted to move her to intensive care. (She was 87, and had been in the hospital three times in the past three months.) We said no, move her to hospice. What is the point in extending her "life" a few more days?
It can be very frustrating when an elderly relative is in an assisted living center or nursing home. The whole system is set up so that they will get maximum care, whenever they (slightly) need it. A visiting nurse would stop by, determine that some additional care was needed, and we would get a call to please take my mother-in-law to the emergency room, yet again.
My 91 year old father in law now has a brain tumor coming back for the third time. He would never live through surgery, but apparently there is some new treatment we could try otherwise. But his mental condition was poor even before the tumor came back--doesn't understand whether his wife left him or died. (She died, two years ago.) What would be the point?
The points of USA over treatment of the elderly and terminally ill:
1) make money providing health services - a distortion caused by 3rd party payers. If people had to directly pay cash for the health services to their own elderly like they have to pay cash for vet care for their pets, most of these services would not exist
2) avoid liability for under treatment - a distortion caused by the tort system in the USA
In the system I work in (socialized) both of these old people would have been tracked to hospice early on with great cost savings.
However, there are still huge distortions caused by people not being responsible for their own health costs.
When injury and illness treatment is free, people are less careful to avoid injury and illness.
Didn't you read the article?
The uninsured get injured and sick more often than the insured. They just don't go until things hurt too much which means higher uncompensated costs for the hospital. The added stress of poverty causes more disease among the uninsured working poor and unemployed. People are healthier in socialist democracies like Denmark because their health access doesn't disappear when they lose a job.
Just the idea of paying for end of life counseling led the well insured right wingers to claim the government wants to pull the plug on granny. Fox News made such discussions taboo.
Taking away the right to petition for redress of grievances has been instituted in some states and there is no evidence it has any effect on health care costs. These high priced judgments are the result of lifetime limits on insurance running out and by folks who don't have insurance. People don't sue the doctors whom they have had long term relationships with even when they make mistakes. They sue because of the mistakes of overworked interns they had just met.
Suggesting we care for elderly family members the same way we do for our pets show how miserly some people are. A very sick dog no matter what its age is euthanized and you suggest in effect the same for people.
Yes, thanks for the clear thinking Thomas.
And for those of you who continue to deplore the money we spend with low odds of success: you tell me, how much money is worth a 10% odd of surviving 5, 10 years? Of being cured? When it's your 10 year old child? Your 45 year old spouse? Your 72 year old father?
Should your decision to save your child depend on whether you happen to have enough money?? Once and for all, yes or no?
We actually MUST think these through as a society. And we won't.
The percentage of the health care dollar that goes to administrative costs with private insurance is between 20-30%. Whether we save that much by having an administrative review process is not known, in my opinion. The experience of every other country in the world suggests not.
Whether we would save a lot more with some sort of public policy that helps with toxic food consumption, toxic air, toxic water and income inequality is known. But how appealing is it to live without fast food?
But isn't there a limit somewhere? How much would you say we (as a society) should collectively spend to extend someone's life six weeks? $30,000? $300,000? $500,000? A million? $10 million? $100 million? $100 billion? Isn't there a limit somewhere?
Yes, absolutely. And medical progress is turning out to be our nemesis. The work now is to have a robust societal conversation on exactly the question you ask.
What really bothers me is saying that your life is worth $10 million, because your father is a multimillionaire and can afford to cough it up, while mine isn't because my dad is only a dentist. Why it's wrong is that it demeans human life. It establishes that, paraphrasing George Orwell:
From there, I believe, there is not far to go to demean all life on the planet, and insist on plundering it precisely because you never know when you might need an extra $10 million.
My family did make the decision to let my father die just short of his 66th birthday. He had inoperable brain cancer and the doctor had urged us to try chemotherapy even though he admitted that the chances of success were small. With one exception our family agreed to just give him morphine and he passed away in less than a week. The point is that another family would choose the opposite of ours which is okay with me. The government or an insurance company should not be allowed to make that decision.
The cost of treatment was not an issue in my father's case since he was a retired postal worker. In effect 100% of his health care costs were born by the federal government and people buying stamps.
Gail, you have my sympathy;we've just been thru this sme type of expeience a number of times in my family.
May I reccomend to you and anyone else in ths situation two books written by medical professionals and considered standard in the field?
They are "The Thirty six Hour Day and "There's a Person in there".
The deal primarily with Alzhiemers disease and the task of looking after a family member afflicted with it, but except for the specific interventions particular to Alzhiemers,the these books are entirely relevant to to the enormous job of looking after any older person as they apprach the end of thier life.
These books are assigned reading in many nursing and social work programs and will help the reader develop the perspective to make good decisions taking into acccount the individual and family circumstances.
In our family when someone gets old and sick we look after them at home until the end if at all possible but the "do not resucitate " order goes on the refrigerator door once it is obvious that our elder is suffering and not much longer for this world.
Worrying about addiction or the ill effects on the health of narcotic drugs when prescribed to someone with a terminal illness is so foolish I could not carry on a respectful conversation with a person who takes such twaddle seriously.
Hold thier hand, tell them you love them ,answer the same question fity times in a day with a smile,and give them thier pain killers!
The doc who wrote this article has his head screwed on straight.
My wife retired from a major health insurance company, so the cost of health care has always been a curiosity. My whole career as a manufacturing engineer was about reducing cost, which engineers in general have done an amazing job of. Manufacturing is about having better machines, methods and materials and using every possible technology to shave the last cent off of cost. Over the last century this resulted in a 90% real cost decline for almost everything in our lives, from electricity to food, long distance telephone calls and a long list of other items. Everything but health care. Part of the reason is that the population has aged, but the other reason is that we do not have active cost controls like seeing lower level medical personnel or having a better education in prevention.
Information technology can help. For instance we could have uniform standards for digital paperwork, both patient records and claims and billing (maybe patients could find mistakes in hospital billing)
and on line diagnostic programs that would allow both medical personnel and patients to compare their own symptoms and vital statistics to database of diseases and treatments.
Paul,
In fact, real costs for treatments that existed decades ago (for example ER visits for asthma attacks) have gone down when studied in detail by medical economists. Real wages in health care have also been declining worldwide for decades. Where I am, nurses get just 2 x minimum wage. Carpenters made more than doctors during the recent housing bubble here. In the 1960s in the USA, 2/3rds of health care money went to doctors salaries. By the 1990s, USA doctors salaries were less than 10% of the pie.
The problem is that we are not measuring a fixed basket of goods and services. New treatments and tests continue to add cost even as the costs of the old treatments and tests deflate. In the 1970s, nobody had to pay for MRI scans, Herceptin, or DNA tests.
This is a problem even in socialized systems such as the one I work in. Population aging makes it worse.
This is a Red Queen's race problem. However, freezing innovation would solve half the problem. In effect my national system tries to do this by keeping new drugs and tests out of the country as long as possible.
I advocate training a group of Health Care Biomedical Engineers, similar to industrial engineers (Taylorism/time motion studies/scientific management). They should work with the public, doctors and insurance companies just like the US Department of Agriculture does with the farmers. They should also be an essential part of Medicare and other government programs.
I am talking about a wide range of interdisciplinary training. They need to understand medicine, diagnostic instruments, and pharmacy and information technology. There are a few engineering programs the concentrate on some of these, but they need to all be brought together, either with one discipline or with teams composed of members with the necessary background.
That very "Information Technology" makes use of hundreds of powerful servers doing the number crunching by being up 24x7 and consuming phenomenal amounts of energy.
IT will only naturally die. There are less efficient, but more effective ways of number crunching. Plus, do we need _that much_ of number crunching when we think the complexity that we've achieved will not stay?
consuming phenomenal amounts of energy....IT will only naturally die.
Bullshit.
Apple's old Newton 2100 used 57mA at (6ish) volts. No idea what the google dev1 phone uses (should check however)
For the sake of argument - lets say 100mA at 5 volts for a device that can communicate (at higher wattage) in a store and forward network and could address an 8 gig SDHC card.
Raw text at 2K a page - 4 million pages of ASCII text. What would the embedded energy for 4 million paper pages?
And that Newton of 10 years ago, or the Google dev1 phone of 2 years ago has FAR more processing power than the PCs of the mid to late 1980's. Well written purposeful code for such platforms would STILL be useful.
You will only be right if somehow Mankind can't make 1.2 Volt CMOS chips anymore.
I will give you the range of somehows are quite boggling. Yet - the production of ICs are a big concern for the military and man's desire for communication seems to stem from man's very DNA. Given the willingness of nation-states to fund military-things - ICs are going to be around for some time.
So as long as man wants to convey information AND tools like general purpose microprocessors with network access are known - many humans will work very hard to keep them.
Youtube, AJAX, and even the MP3 podcasts may have to go in an energy constrained world - but as long as phone lines worth of bandwidth exist - things like UUCP can keep a network going.
(And if one believes the halfpasthuman "time machine" project - "the internet" as we know it goes poof by 2013. Could be war, could be replaced with 'something better', could be stifled with acts of law)
An excellent article, and confirms many of my own thoughts on the matter.
Ultimately, as long as a country has 1) a basic vaccination program and obstetrics and 2) no particular social ills such as AIDS (sub-Saharan Africa) or prevalent alcoholism (Russia / Ukraine), then it is virtually guaranteed a life expectancy in the 70's. Even the best healthcare would only barely nudge it into the low 80's.
This means that as long as we don't get huge wars or Malthusian crises in the post-industrial age (something I'm not too sure about), the humanitarian consequences need not be too severe.
I would expect that the huge wars and internal social stresses will precede any Malthusian crisis. The chief point being is that only during the surplus resource days of the oil age has general survival been seen as desirable. It is a feel good luxury, like organ transplants for felons. Never before in history have people been able and willing to provide so much largess to strangers. It is not the norm.
The "eugenics" practices of 1930s Germany involving forced sterilization and euthanasia are notorious. What is less often remembered is that the USA also practiced forced sterilization. It was done to mental patients and welfare mothers were sometimes sterilized without consent when they were hospitalized for childbirth. As for withholding health care of treatable illnesses, google "Tuskegee Experiment"
There have been many campfire posts on the thermo/gene switch. When other people, outside one's immediate social group, are seen as competitors. That is how most people have lived for the last 100,000 years.
People will come into conflict as soon as they see their own circumstances deteriorate, even if food is still abundant. Why should one wish for strangers to live longer and continue competing with one for shrinking supplies of gasoline? So why would one wish to pay for obstetric care for strangers (competitors)? General longevity will decline, because people will want it to decline, for everyone except their own family and close friends.
Interesting article and great post by MicroHydro. I'm an internist myself, though a bit fresher...finished residency in 2008, right as the crash was unfolding. Been lurking here since then, but this is my first post.
One of the many overlooked parts of our system that is collapsing-we just don't know it yet-is healthcare. Sure, everybody talks or comments about a healthcare crisis, or about this or that plan being announced or scrapped by our politicians, etc., most of which is nothing but random noise. At the same time, healthcare constitutes 17-18% of our GDP and is one of the only sectors growing jobs. So is healthcare in crisis, or is it booming? The moment we ask this question is the moment we can see how bipolar the whole discussion is. Once we put on our handy post-peak, oildrum looking glasses, we can see what's really going on-that modern healthcare constitutes one of the last bubbles of the pre-peak oil age. At some point, the costs of all of it, for the technology, the workers, to keep the whole thing going...all the hospitals, ER's, offices, clinics, ambulances, drugs and devices based on plastics...will overwhelm the flow of the money/energy from the remainder of the productive economy to service it, and then healthcare will deflate...then all of our young people can look forward to being drummed into the military.
To some extent, we see this happening already. The cuts in Medicare rates that are always one more year into the future are soon to happen...and when salaries of middle class profession people go down (and there are millions of them), take a guess as to what will happen to the econony. I've worked at hospitals, which happen to run beautifully, where the surrounding neighborhoods look like a second world country. How long can these hospitals operate? I suspect they won't be around 20 years from now.
At first, the decline of modern healthcare won't do much to alter population health or life expectancies...for all the reasons mentioned in the article. But what happens when there are no longer antibiotics or vaccines? That's a whole different ballgame than going without gastric bypass or hip replacements. And it's coming...we just don't know when.
I too, for the moment, am working part time and, day by day, drying to make sense of things and come up with a game plan for survival. Good luck to everyone, and I'll definitely post more in the future!
Welcome OS, and thanks.
I am in an (at best) second world environment. The roofs of houses are corrugated iron, central heating and AC are almost unknown, and mosquito screens are non-existent. Thank goodness we don't have dengue fever or malaria (yet).
So I have the answer as to what happens to health services in a second rate economy, and it isn't pretty. The good news is that there is always unlimited work available for doctors and nurses. The bad news is that the working conditions and pay are bad and getting worse. There are hundreds of unfilled positions for doctors.
A recent study found that the 3 most hazardous national occupations for workplace violence were transport workers (taxi & bus), doctors, and nurses. Yes, it is more dangerous to be a doctor or nurse than a (legal) brothel prostitute. That is what happens when one is exposed to drunks, gangsters, and meth addicts at all hours.
(I am reminded of a story in National Geographic, perhaps a decade ago, about Russia. One of the people depicted was a woman doctor in Irkutsk. She still worked for the government but had not been paid in months. She was basically homeless and lived in a lean-to shack she had built by the railway. She worked with almost no medicines or supplies and survived on food donations from her patients. So much for higher education being a guaranteed path to riches, LOL. )
My advice is don't worry about survival. Life is a terminal process, nobody gets out alive. Come up with a game plan for living life fully in the here and now. Sing a song, maybe write some. Read good books. Play some sports. Write a poem. Share good meals with friends. Paint some pictures. Fall in love, or at least enjoy some lovers.
As Lady Gaga said, "Just dance, it'll be ok, da da do do just dance, spin that record babe, da da do do just dance"
"drunks, gangsters, and meth addicts at all hours" - exactly why the retention rate at the ER in the hospital where I trained was so low
As far as living in the here and now...good advice to be sure, and I am trying...but where are all the peak oil aware folk to have a beer with?!
Try the Fort George Brewhouse and Pub, Astoria, OR. You will find many congenial people (and some not so much.) Let me know when you are coming, I will have a Vortex with you (best beer on earth.)
The problem with medical care which has not even been mentioned once here (perhaps alluded to) is that it is no longer medical care we are speaking of, but a commodity, called "healthcare" which is subject to the same forces as any other commodity, like pork bellies or corn or oil.
Doctors and nurses and all the other helpful people need to be paid for attending the sick, or advising the well -- but commodifying those activities, securitizing them, selling futures on them, well, that leads to all the distortions you see.
My town of 10,000 people in a population area of possibly 30,000 (including the two other towns on the North Coast) has 2 MRI machines, at least two advanced CT scanners, and the two adjacent towns (each about 25 miles away) also have their own hospitals and MRI and CT machines. That strikes me as the same level of decisionmaking as subprime mortgage activity -- just sell it, get your money out and let someone else clean up the mess.
I honestly don't think we were that much worse off 100 years ago before there was such a thing as "health insurance."
I'm perfectly acceptive to the message, about rather minimal effects, however I suspect some of the stuff that we take as pretty routine actually helps a great deal -perhaps these are not included in your two month figure:
(1) Childbirth: this used to be pretty dangerous. Even for the well to do a couple hundred years ago, getting pregnant at age forty was considered to be a death sentence. So I suspect this area of medicine contributes substantially to average longevity.
(2) Antibiotics, bacterial infections either from injuries, or because in our modern organized societies the ability of diseases to become widespread is so much greater than in low density hunter gatherer societies.
(3) Basic public health, sanitation mainly.
(4) Vaccines, which have eliminated or controlled a lot of the diseases we've picked up since transitioning to high density societies.
(5) Trama treatment in the case of serious accidents.
I completely agree with the author, and remember a surgeon-general quote from 20 years ago where he estimated that medical care accounts for 10% of health outcomes. I spent 20 years both doing individual medical care, studying public health and child abuse prevention, and reflecting on the life circumstances of my homeless patients.
One thing to remember is that we are stuck. We do in fact have more medical conditions, which then result in more medical expenditures. These expenditures are not just a waste. Without them, I would guess our health status would be worse yet. For example, the premature babies that so affect our life expectancy numbers would just die.
When I was researching a paper on "Health, Wealth and Medical Care", I came across someone's PhD thesis, where he correlated states' health expenditures and health status measures. Of course, the more states spent on health care, the worse the health status. And that's NOT because most doctors make most people sicker.
This means that in order to fix the problem, we have to adopt public policies that address income inequality, neighborhood incentives to smoke and eat fried GMO-fed sick animal parts, whatever drives pregnant women to use drugs, whatever causes so many babies to be born premature (the drugs only account for some of it), whatever causes so many young men to try to murder each other, etc, etc...
How we would do this in a society so entrenched in spending 17% of the GDP on medical procedures and expensive medications is unclear.
Collapse offers hope for complete restructuring.
Of course die-off will be worse than voluntary restructuring ever would have been.
i'm a trained geriatrician and would like to clarify a few things that i learned recently to my surprise. human life span has not changed a single bit for atleast in the last 100,000 years. its fixed at 85 yrs. animals studies have confirmed the same observation. note that life span of a species is not the same thing as its 'life expectancy'.
secondly, vaccinations provide no gaurantee of immunity against any disease. they are over rated. on the contrary they are all neurotoxic (especially in infants) and can potentially lead to autoimmune diseases later in life. the only reason docs recommend is because industry says so.
in my opinion, the key to health is to eat less, mostly plants (as michael pollan says) cleanliness and stay away from pharmaceuticals.
Agree, the human species natural lifespan has not changed. Although I am surprised that you would be surprised by that. There might be a weak genetic selection for post reproductive survival, as children could be helped by living grandparents, but no reason for genetic selection for a lifespan past 85. Of course, actual life expectancy has gone up by about 2 years every decade for decades. Due to the wealth of the oil age, more people get to live to senescence.
As for the future: "Rapamycin fed late in life extends lifespan in genetically heterogeneous mice."
http://www.nature.com/nature/journal/v460/n7253/full/nature08221.html
Whether this is a good thing or not is a matter of opinion.
I am also a medical doctor, an eye surgeon. I completely agree that life expectancy of a population depends much more upon lifestyle than health care expenditures. I would also add that dependence upon cheap fossil fuels in some ways reduces population health. How?
Humans require about an hour a day of vigorous activity for good health. Fossil fuel replacement of muscle power has enabled most Americans to eliminate vigorous activity. SUVS replaced walking to work or school, blowers displaced rakes and snow shovels, elevators quieted stairs. And when Americans do get exercise, it is usually on a FF powered machine in a FF powered gym.
Cheap FF have also given us cheap sugar and meat. FFs are processed into synthetic pesticides and fertilizers to produce cheap corn which yields cheap sugar (high fructose corn syrup) and cheap meat (from corn fed to penned up cattle). The combination of inactivity with cheap sugar and meat, produces obesity, diabetes, cardiovascular diseases, and cancers. And also raises debt by increasing disability and health costs.
So, many choices that make us healthier, also reduce FF consumption and climate change.
Great points...and my congrats on your decision, made for whatever reason, to become an ophthalmologist. Can you imagine life as an internist these days?
Don't knock the life of an internist. It is one of the most interesting jobs in the world, it brings you into intimate relationship with others in ways (don't misread that in some salacious or inappropriate way!) that no other profession can possibly do. The range of human possibilities is nearly infinite -- one doesn't have to confine oneself to treating diabetes in rich, overfed, smug, entitled ones -- there are a lot of people out there who need and appreciate the help you have to offer. And you can get paid for it! Maybe not so well, compared to an eye surgeon, but you won't starve.
And in any case, it beats flipping burgers.
Great post and supporting visuals. I have a major disagreement, however, with the following sentiments expressed in the article:
"Like everything else in our artificial modern world, healthcare and energy problems are really economic and social policy issues."
"Science is the most powerful way to look at the world."
"Obesity is a social problem, and especially affects poor and minority people inside rich countries."
"It would be cheaper and more effective to treat many diseases as the social problems they really are. Good societal living conditions are the ultimate preventive medicines. Teach girls to read, thus saving the world."
I would wager that all of the above are moral/psychological issues that become social issues. Science is only one way of looking at the world and just because it is the most destructive way, does not mean it is the most powerful. Many illiterate cultures, dying off not due to self-implosion, but rather to encroachment of the "civilized", lead happy lives. This 'happy' part, so damn difficult to quantify or qualify, gets dropped so often since it clearly is easier to discuss "mortality rates". The fact that so many follow-up posts focussed on adult, infant, childbirth, etc. mortality rates simply illuminates a cultural phobia with death. The concept of death in our culture is not shared by all and could be something that needs work along with other aspects of healthcare. As an addendum to the literature citations for the article, Google the Center for Disease Control links to the Adverse Childhood Experience study indicating the association between such experiences and later mental and physical health problems (Kaiser Permanente study by Anda and Felliti).
With regards to a few other follow-up posts:
From WNC Observer;
"Prevention and control of infectious diseases. These can sweep through an entire population and cause a massive die-off, and now we have bioterrorism to worry about, so this is actually not just a health care issue but also a homeland security issue. It is absolutely, utterly stupid for people to go around unimmunized because they cannot afford the vaccination. It is also absolutely, utterly stupid to define and defend personal freedom in such an extreme way as to give contgeous people the absolute right to spread infections freely. We don't let people go around spraying machine gun fire at crowds, we shouldn't let infected people spray deadly germs at crowds either. Quarantine is an effective tool, let's use it if needed."
I'm a healthy, PhD virologist and you know what??? I'M not getting any of the friggin H1N1 vaccine or any other at this point. Although I don't do this as a wish to become the next "Typhoid Billy", I also don't feel that maintenence of the precious human population to be top priority right now. We spend so much time worrying about this and that health for humans while the planet croaks. On another point, we may not "...let people go around spraying machine gun fire at crowds", but we also don't blink when, in the name of the economy, we crowd millions into unfit work places that reduce their health as well.
and Paranoid added: "Of course die-off will be worse than voluntary restructuring ever would have been."
As I indicated above, I can think of several restructuring scenarios that would be far worst than die off.....
BWB
right on, Bad.
The world is waking up to the notion that SUV's and fighter jets and the rest will buy neither happiness nor improved life expectancy. It just takes a while for new ideas to seep in, even the bad ones. The Chinese allegedly invented gunpowder hundreds of years before anyone figured out how to use it destructively -- and of course, they knew perfectly well how to cast cannons, had they chosen to.
It might take another 100 years, but I believe that the Schumacher ethic (small is beautiful) will ultimately prevail.
Also, vaccines make some sense in some situations -- as a "solution" to anything, they are useless, except to make profits, extend the power of the police state, and as leverage to divert public resources to private gain.
I don't see where uor anti-vaccine attitude comes from. Vaccines are an essential cornerstone of public health, even if they are not totally effective on a individual basis. Consider the case of a virus which in an unimumized population every sick person infects two others. In epidemiology this would be described as having an R0 of 2.0, an any infection introduced into this population is likely to create a pandemic, infecting a considerable fraction of the population before it dies out. Now say we have a vaccine that is only seventy percent effective, and we administer to seventy percent of the population. Now recompute R0:
the thirty percent unvaccinated contribute a total of .6 to R0. The seventy percent that are vaccinated are still thirty percent susceptable, so they contribute .3*.7 = .21 to R0. The total R0 for this population is now .81, so introduce an infection, and it spreads thusly
1 infection begets .81
.81 begets .81*.81
.81*.81*.81 begets .81*.81*.81
...
the series converges at roughly five total infections, versus a large fraction of the population for the unvaccinated population.
The inescapable conclusion is that vaccination is a responsibility of all the citizens. That is part of the bargain of civilization, you can't do just as you please, you have to take into account your effect on others, and on the system as a whole. Now I know in the US we have this fixation on rights and individual freedom, and we slight collective responsibility. Without the later the former is really useless (life will be brutish and short). Like all things we have to find a decent compromise.
Of course, in light of population overshoot, maybe the thing to do is not immunize. Population reduction in a fair and unbiased package, killing the rich and poor alike(though not perfectly alike..) And probably better than mas starvation.
I thought this press article was interesting. An excerpt,
Something I thought equally interesting was the suggestion of a connection between soil fertility and health in an online publication by Steve Solomon. At the link, scroll down to the section Lessons From Nutritional Anthropology.
At least twice in your article, you said, "The bad health of Americans isn’t doctors' fault."
Yes, yes it is.
And just to be clear: The bad health of Americans IS doctors' fault, first and foremost.
The medico-industrial complex has become nothing more than another wealth extraction mechanism in our hypercapitalist society. The premise may be health care, but the reality of the situation is that you're extracting a hell of a lot of money from our society, and as you described in your own article, we're not getting much of anything to show for it.
A person who takes money in return for promises that in reality go unfulfilled is generally considered to be a con man, isn't he?
How on earth can this NOT be your (collective) fault? Because so many Americans are so gullible that they let you do it? That may mean that you can get away with it, but it doesn't make it right.
Psychologically you may be able to talk yourself into believing that "the problem" lies elsewhere, but seriously, it doesn't. If you want to see where the problem with American medicine lies, go to an AMA meeting... or look in the mirror.
And if the system is to be reformed, who do we look to for guidance on how to fix it? Doctors. A classic fox-guarding-the-henhouse situation.
Meanwhile, just about all doctors, including you, continue to deny responsibility. "Oh, it's not *our* fault!" Yes, it *is* your fault.
America's dismal medical industry will NOT be reformed until the patients realize that doctors' motives are not as pristine as they think they are, even if doctors themselves believe that their intentions are good. Society should be making demands of the medical industry, not the other way round.
I'm also convinced that we're putting the wrong people through our medical schools, though that argument is probably too long for this comment. But, a short thought experiment: if putting straight A students through med school gave a population an average lifespan of 75 years, but putting B students through med school gave a population an average lifespan of 85 years, what grade would *you* want your doctor to have gotten in calculus? The best doctor who I *cannot* see because the system is broken or because he has 3000 patients and the HMO wants to minimize its loss rate by limiting patient visits to 15 minutes (and since the doctor is already running late, that translates to *five* minutes) is not as effective as one who bucks the system and condescends to spend some time with his patients and find out what their actual medical issues are so he can address them. Grades are a poor proxy for ultimate career effectiveness. (Disclaimer: I work around a lot of premed students. Observing them... explains a lot.)
The reason medical care doesn't help society more than it does is that we have a medical industry filled with very smart, very ineffective doctors who have been culturally programmed by their medical industry to maintain the status quo, and not question any of their basic assumptions about the "healing" profession.
And you should all be ashamed of yourselves for that... but you have been selected and bred for large egos to prevent that from happening.
And your patients have been culturally programmed to trust your profession. Trust which is, when the evidence is looked at objectively, probably not well deserved.
If you, personally, Dr. Rock Climber, want this state of affairs to change, the *first* thing you need to do is to start accepting responsibility for your own industry's flaws. And learn to see past the blinders that were installed on you in medical school.
The blindness you describe in your article... is your own blindness, I think. The dark matter is nothing more than a deeply flawed but thoroughly entrenched culture in a medical industry that fails too see that fact... but profits anyway.
And, really, in a hypercapitalist world, why try to change things when you're still making money hand over fist?
sarahannalien:
If either you, your family members, or one of your friends has somehow been wronged by somebody in healthcare, then that's unfortunate and I can understand your point of view, and your apparent anger. I can't however, as a physician apologize for the actions of others...and I seriously doubt if I was involved.
Believe it or not, almost everybody in healthcare, and that includes most physicians, are aware of the many problems. Just like people who work for ExxonMobile or Saudi Aramco are aware of peak oil. The reason that nobody works for a solution in healthcare is that there is no solution there to be found.
If you, like everybody else in these grand United States, have your own personal "fix" for healthcare, go ahead and lay it out. If it's anywhere near as misinformed as your post, I would have no problem shredding it to pieces, though it may take a page or two.
Well, as devils advocate I'd think a good place to start would be by requiring doctors to report mistakes, misdiagnoses, and reporting the frequencies of recommending procedures that prove to be unnecessary--or simply useless. A bit of transparency like this might offer the rest of us the information by which to suggest to reform the system. There's very little transparency in the system, very little information provided as to tell who's a good doc and who's a hack. That's a professional privilege almost unheard of in any other industry.
Once we resolve that competency issue, I'd like to also be able ask, questions like, "Uh, so what is this going to cost me?" and get an answer. That would help too.
Anyway, opinions on that? My pop was an undertaker, and I know full well we buried a lot of whoopsies.
Comparative effectiveness studies and rankings have been performed on hospitals for some time, and they have dramatically improved the quality of care at hospitals (at great cost, of course). I think alot of this information is available, but to be honest I've never really tried to look for it. Moreover, you can get information on any licensed physician from state medical boards, including whether they've had a successful lawsuit against them, disciplinary actions, etc. I suppose it's possible to go further than this, but it's awfully tricky, given that medicine is an art based upon science, but an art nonetheless. To give an example, suppose the metric was how well a physician controls their patient's blood pressure, with goal 140/90. Physician A spends five minutes with his/her patient, prescribes 5 pills, all of which have side effects, and their bp reading is 139/89. Physician B spends fifteen minutes with his/her patient, gains their trust, instructs them to eat better, walk more, cut back on salt, and prescribes 2 pills, and their bp reading is 141/91. Based only the bp metric, Physician A is better, which shows the absurdity of only using that measurement. Which then introduces a question...which measurement do you use? Cost is awfully difficult to measure, though we know we are doing horribly in the United States.
As far as whether the public should have this info...do you think Joe Six Pack can understand the complexities of healthcare anymore than I can understand how much oil is being produced by Aramco and how they are doing it? I seriously doubt it.
Again, alot of this is academic as modern medicine, as we know it, is toast. Which is good, or bad, depending on your view. Good if you think we'll be walking/bicycling, drinking green tea, driving electric cars and breathing fresh air, and no more greedy insurance companies or doctors. Bad if you think that the spread of HIV and TB, untreated pain, depression, alcoholism, no vaccines, mother's dying at childbirth, life expectancy dropping, and a human population of 6 billion being reduced to 1 billion in half a century is anything to be concerned about.
That's a sensible answer, but I'd still suggest that some of us are intelligent consumers of medicine. I've got a degenerative condition myself and the fact is I'm often much more informed than the doctor I speak to, which is rare, as with a pre-existing condition I have no medical insurance and rarely can afford treatment. It would save me a buck or two to be able to know ahead of the time whether the guy I was hiring was competent or not, or rather if it was just smarter to buy medications from Central America. Most always, it's the latter.
Which, of course, is why many knowledgeable people by-pass the American system and go to Singapore to get the cutting edge work done for pennies on the dollar. And insurance companies, if you're lucky enough to have insurance, will increasingly support such.
Or get medicines from the local vet, which I do too. That helps.
I think it's a shame and disgrace on our society that you can't get health insurance or good treatment in the U.S., I really do. IMHO, all of this reflects the ongoing peak oil collapse, even if some of the problems predate peak oil. What is on the horizon: basic universal health insurance and greater transparency and accountability in medicine, or endless resource wars in the Middle East? I certainly don't mean to either trivialize or overgeneralize, but I think that to suggest there are solutions to healthcare is indirectly to suggest that there are solutions to peak oil, which I don't believe there are. Though every day is a new day and I'm always open to possibility.
Best statement of the thread. With all due respect to Paul, the efficiency experts, time and motion study people and IT people have been all over medicine like flies on faeces for at least 30 years. Despite that, USA consumer dissatisfaction with health care, health care costs, and real wages and working conditions for health care providers have been worsening the entire time.
In fact, my job has been made so "productive" that no colleague of my generation had children go into medicine. People don't like working in a sweatshop. When you have to see 20 people before lunch, that is what it is.
Every political solution suggested in the USA already exists somewhere else. While many models are more cost effective and simpler than the USA one, the same problems are progressing in every health care system including the cut rate socialist system I work in now. Older populations, worse health habits, and coping with the cost more expensive new technologies.
This is the collapse of a complex system, as per Tainter.
It is also occurring at this time due to peak oil. in the (near) future, we will all be poorer. That means the health care system of Zimbabwe is the future.
You could say that a rational personal response to peak oil is to recognize that there is a societal value to your energy-behavior, and to then begin to behave in a way that reduces your burden upon society and increases your personal freedom within the constraint; that is, you reduce, conserve, reuse, etc.
You could also say that a rational personal response to the healthcare problem in the US is to recognize that there is a societal value to your health-behavior, and then begin to behave in a way that reduces your burden upon society and increases your personal freedom within that constraint; that is, you eat healthy, exercise, eliminate unhealthy habits, etc.
There have been a number of good books lately on health care and its discontents. One is "Hippocrates' Shadow" by David Newman. Another author who has several books is Atul Gawanda.
Being married to an RN of 30 years experience has given me a view into the 'seamy side' of medicine. I do believe that there are solutions to US medical system problems, but not the political or social will to implement them. My sympathies go to all the many physicians who went into the profession with genuine desires to help people, only to find themselves in strait jackets of the medical status quo, and a system (if it can even be called a system) that is in thrall to the pharmaceutical and insurance industries, not to mention the hospital systems.
There are so many examples in the developed world of health care systems that we in the US could learn from that it is utterly tragic to see us going the opposite direction and watching things get worse and worse.
My "fix" for our notorious healthcare system, personally, is to very intentionally have no need for it, and its worked fine so far. I don't smoke, rarely drink, I cook all my meals as healthy as might be expected, I get a couple of hours exercise a day in addition to having a fairly physical job, my height-to-weight ratio is very good.
At 45 years of age, I feel very fit and healthy, and can say that my own experience tends to reinforce what the Dr. says - its not the fault of the healthcare system if people are not healthy; on the contrary, it is much more how you choose to live. Of course society influences that to the extent that poverty and status become factors, but in any case the healthcare industry has no power to make people stop drinking and smoking and eating themselves to death, and no power over depression and despair.
Ducky for you if your genes permit it.
You still minimize the "personal choice". Genetics have very little to do with whether a person smokes/drinks/eats him or herself to death; it is a matter of choice.
I've lived long enough to watch friends who grew up with the same influences as me ruin their health with careless and persistent bad habits. The two common things they lacked were, first, any concept of the personal value of health, and any concept that their health had a societal value.
I perhaps minimize that because, from my personal experience, I was born with a condition. Not all of us are born vital. Some of us become vital in spite of that, which is a heroic endeavor. All I'm asking for is access to medicines, commonly available, for a treatable condition. Nope. I've got to kiss the ass of the priesthood at 300 bucks an hour in this country. And pay 10 times the global going rate after I've been blessed with a prescription. By someone who knows less about the condition than I.
That's one situation where I wish we had universal health care. To some extent I think that if people cared a little more about their health then the system wouldn't be sucked dry by "elective" conditions, and we could easily offer treatment for congenital conditions and other problems that nobody deserves to spend their life struggling with.
I have to admit what you are doing is a solution and will serve you well, whatever happens and whatever interaction you have with the healthcare system. I would just add that it's a good idea to have health insurance. Not to vouch for the health insurance industry, which is doing just fine, but you want health insurance for the same reasons you want property insurance. Your body might need work in the future, and it might be expensive.
As far as health insurance, I'm afraid I'm in the same boat as too many people in the US - priced out of the market. My employer would offer it if he could, but he can barely afford it for his own family. One reason I say "its worked so far"...
Yes, I've been wronged *repeatedly* by the healthcare industry... as have my family, my friends, and... well, very nearly everyone I can think of off the top of my head. Even *my* doctor, believe it or not. The first time it happened to me, I shrugged it off because, hey, anybody could make a mistake, right? But the third or fourth time someone nearly kills you and/or takes away a year or decade of your life due to a simple but undiagnosed and untreated illness... or negligence, incompetence, inattention, ignorance... or simply just not giving a damn... well, after that, you just start asking yourself the harder questions. And when it's not one doctor, or two, or three... or one hospital or two... but pretty much *everywhere*, then even simple incompetence is no longer a viable explanation. There has to be a systemic flaw somewhere.
My conclusion, after looking at the issue in some detail, and a lot of thought, is that the Emperor at this point is not actually naked, but very nearly so.
I'd try to explain in detail; unfortunately, I haven't had time to write that book yet. Perhaps if I live long enough, I'll find the time.
The comparison with peak oil is, I think, not apt. While there are definitely obvious energy issues both in our present and in our future, the oil industry still sells a product that can be converted into useful energy that can do useful work. I put the gas in my car, and it goes. Fair enough.
The healthcare industry, all too often, charges money for goods and services that lead to no better health than would have been had without said goods and services. If I put gas in my car that caused it to *not* go, I think I'd have good reason to be angry, don't you?
Yes, I do have a "fix" for American healthcare... unfortunately, the closest historical parallel to *my* plan is probably the French Revolution, because I doubt doctors will give up their current power and privilege willingly.
You may think that you are aware of the problems... but what I'm trying to say, in my angry and frustrated way, is that ALL doctors have deep psychological and cognitive blind spots that prevent them from seeing some of the real problems... and socioeconomic and cultural issues that would prevent them from addressing them if they *could* see them. (Although, I think that when *my* doctor was treated badly as a *patient* at the Mayo Clinic, he perhaps began to see the light.)
To me the more interesting issue is why patients don't demand both better and cheaper service.
If I'm not feeling well, and the first appointment I can get is six weeks later, and when I get to the doctor's office I'm kept waiting for an hour and a half... and then he spends five minutes brushing off my complaint before sending me on my way with absolutely *nothing*, helpful or otherwise, and then bills me $150 or more for that "service"... well, it seems to me that any normal person would have a problem with that. And yet, I've received that level of primary care from more than one doctor, at more than one hospital, and with more than one insurance plan... as have many, many people I know. Why do we put up with it, as patients? Clearly, the patients have serious blind spots of their own.
You said, "...there is no solution there to be found." As Master Yoda said... that is why you fail.
I will agree with you that the current system cannot be fixed. It must be replaced in its entirety. And the new system has to have a better balance of patient-power to physician-power. At the moment, we have a sort of "temple-style" system: you prostrate yourself at the high temple of medicine, make your offerings, and just hope that you are granted a boon. As a temple priest, your ability to see things from the patients' side is a bit constrained. As patients, we are largely powerless, particularly when we are sick, vulnerable, and not lawyered-up. (And if, after several decades of poor medical care, we become a little more insistent about receiving adequate care, we're labeled "problem patients" and looked down upon with annoyance. But our heath often improves, and as I recall statistics actually bear this out; I read a study somewhere that said that (to paraphrase) aggressive, demanding patients who probably annoy the hell out of their doctors actually have better survival statistics than the meek, compliant ones. Sorry, I don't have the reference at hand at the moment.)
Any effective replacement system must be more egalitarian, so that patients can recognize poor service and take their business elsewhere as a result, and so that doctors will feel threatened enough by the loss of business to keep their industry from spiraling out of control again. At the moment, the medical guild system successfully constrains the supply of doctors, and maintains a monopoly on robust scientific care, thus keeping prices high... and when one sucker gets fed up and leaves, there's still a healthy supply of gullible new patients waiting in line, so there's no danger of loss of income or prestige due to poor service or lack of effectiveness. There's no particular incentive for success, which is clearly a problem in its own right, and often no penalty for failure, either.
But, as I said, I really don't think physicians will give up their current power and prestige willingly... and most of their patients still think the Emperor has a fine, fine new suit.
Oh and Doctor, if I ever wind up in your office, and I wind up screaming at you... FYI, it's not that I'm a jerk... it's iatrogenic PTSD. Twenty years of poor medical care, and twenty years of trusting a multitude of doctors who, as it turned out, came nowhere near deserving that trust, have left plenty of scars, both physical and emotional. And if you want my respect, you'll have to earn it from scratch; I can no longer grovel at the door like your other patients because *you* went to medical school and I didn't. I *am* sorry about that, but *your* industry did this to me, and I am sadly powerless to fix it... and as your industry's monopoly on medical care ensures that I'll have to be periodically re-victimized whenever I need medical care, the system has been carefully tuned to ensure that I'll never be given the opportunity to heal.
Perhaps this will help you understand why I'm not only critical, but also very, very angry.
"But the third or fourth time someone nearly kills you and/or takes away a year or decade of your life due to a simple but undiagnosed and untreated illness... or negligence, incompetence, inattention, ignorance... or simply just not giving a damn... well, after that, you just start asking yourself the harder questions."
-You are still here right? Still have a hearbeat, still breathing, able to sit up, able to type, able to see, able to read, able to think and post something on an internet forum? While I sympathize with any medical problems you may have, doctors routinely...every single day...deal with patients who can't breath (resp. failure), no heartbeat (heart attack, cardiac arrest, arrythmia), can't think (dementia), can't see (cataract, macular degeneration), can't type (neurological disease, arthritis). I hate to burst your bubble but we don't deal just in midiagnosing and failing to treat the common cold.
"I'd try to explain in detail; unfortunately, I haven't had time to write that book yet. Perhaps if I live long enough, I'll find the time."
-Let me know when you do, so I can read and review it
"The comparison with peak oil is, I think, not apt."
-I wonder how doctors and nurses get to work; I wonder how hospitals are supplied; I wonder where pharmaceuticals come from, and how they are distributed; I wonder what makes ambulances run...surely it's not oil! And surely it's no problem if oil supplies decline and prices go up! Nope, peak oil must not be relevant to health care at all.
"Yes, I do have a "fix" for American healthcare... unfortunately, the closest historical parallel to *my* plan is probably the French Revolution, because I doubt doctors will give up their current power and privilege willingly."
-Certainly more interesting and juicy than anything Congress can come up with, I'll grant you that; But don't you think you should go after the CEO's of insurance companies first?? That'll buy me time to get out of medicine and pretend I never got an MD!
"Although, I think that when *my* doctor was treated badly as a *patient* at the Mayo Clinic, he perhaps began to see the light.)"
-I've been a patient myself more times than I can count; never once had a problem with anybody providing me with care; admittedly, I've never been hospitalized; though my mother has, with breast cancer...she got surgery, radiation, and chemotherapy, and is still alive today because of it...care to ask her about what she thinks about medicine?
"If I'm not feeling well, and the first appointment I can get is six weeks later, and when I get to the doctor's office I'm kept waiting for an hour and a half... and then he spends five minutes brushing off my complaint before sending me on my way with absolutely *nothing*, helpful or otherwise, and then bills me $150 or more for that "service""
-Hmmm...I think I'm unhappy with this Windows software I'm using crashing all the time...what are those monkeys at Microsoft doing giving me a product like this!! And the last time I was at the supermarket, they didn't have fresh oranges!! And then, to top it all off, I drove to the gas station and gas was over $3!! Who do these people think they are????!!!
"You said, "...there is no solution there to be found." As Master Yoda said... that is why you fail."
-Admittedly I'm a Star Wars fan myself...but you know that a post on the OilDrum, ideally a forum for serious discussion about peak oil and resource depletion in the real world, has jumped the shark when there is mention of a little green guy conjured up by a filmmaker more than 30 years ago
"Any effective replacement system must be more egalitarian, so that patients can recognize poor service and take their business elsewhere as a result, and so that doctors will feel threatened enough by the loss of business to keep their industry from spiraling out of control again."
-I didn't know that I could force patients to be mine, all mine. Do you know something that they didn't teach me in medical school or residency?
"There's no particular incentive for success, which is clearly a problem in its own right"
-How about recognition by peers, respect of patients, sense of accomplishment at seeing diseases cured and human function restored...and last, but certainly not least, money (ah, but that's probably a problem)
"and often no penalty for failure, either."
-How about losing my license and not being able to practice medicine ever again?
"Perhaps this will help you understand why I'm not only critical, but also very, very angry."
-Not really; but then again, this is just an internet forum, and I'm just a random person, so you don't have to get specific
If you despise me for my sarcasm and mean spiritedness, so be it. Just bear in mind that although I'm a physician, I'm on the oil drum to talk about peak oil and its effects on everything, including healthcare...I just don't think rants or sob stories are very helpful...if you have anything serious or insightful to say (or if you ever get around to writing that book), well then I'm all ears and will respond more gently
You are banging your head against an immovable force. Your comments in various posts make me feel you have to 'apologize' for the profession. You can't do it. Don't apologize for things you didn't do. You don't have to apologize for the acts of your profession, because on balance, it provides good care to most people. Some people have bad luck. Some people let that color their entire lives and they want to spread the poison around. Don't let them. IGNORE IT. There will always be people who have had bad experiences.
I am also a doctor. We all make mistakes, for which we pay, either with feelings of guilt, or sadness, or sometimes even with cold hard cash. If we are good at our profession, we learn from those mistakes and try not to let them happen again. We have to carry our own guilt; we can't carry guilt for the whole profession. So, let it go.
Don
"If you despise me for my sarcasm and mean spiritedness, so be it."
Oh, no, not at all... far from it. I learned the hard way, over many difficult years, that you can't actually tell a doctor anything, because he's been trained to believe with unshakable conviction that he actually does already know it all, and anyone who questions that premise is a fool. And I've come to believe that, deep down, all doctors also all know it isn't true, and live in perpetual fear that they will be found out... which I suspect is why they tend to act angry, mean, and sarcastic when they are questioned. You're acting normally, and I'm not offended or surprised.
Since I don't have my own book to offer, might I perhaps offer this one instead:
Alien Worlds: Social and Religious Dimensions of Extraterrestrial Contact
This may seem to be an exceedingly odd choice, but perhaps I can explain.
The book is basically a series of essays about UFO cults: where they come from, the nature and possible origins of their beliefs, and the nature of the thought process that goes into sustaining those beliefs.
What I found fascinating is the notion that people experience a peculiar but more or less ordinary phenomenon, like, say, sleep paralysis, search for meaning for the experience, and, through the peculiar lens of their subculture and belief system, conclude that they are being probed by aliens. Or they see an event in the word news, like the fall of the Berlin Wall, and are confident that this is evidence that the Space Brothers are working behind the scenes on the ethereal plane to bring peace to mankind. (Apologies to any Unarians if you feel I've mischaracterized your beliefs.)
Now, to us outsiders, this seems wildly outlandish, of course. And, unlike the major religions, they haven't had hundreds or thousands of years of experience to lend their beliefs a patina of credibility. So we see them as weirdos.
But, as it turns out, cultures which don't have a UFO mythos use a different cultural lens to contextualize those same experiences in terms of their own particular mythos.
What I found fascinating about all this is that, despite the fact that both the believers and the beliefs seem very weird to us as outsiders, the underlying thought patterns and experiences are really pretty common... even in medicine.
Consider, for example, this list I found on the page for "Cults" on Wikipedia:
http://en.wikipedia.org/wiki/Cult#Mind_control
1. People are put in physically or emotionally distressing situations
... I gather that med school is considered to be "difficult"...
2. Their problems are reduced to one simple explanation, which is repeatedly emphasized
... but, we're helping people!
3. They receive unconditional love, acceptance, and attention from a charismatic leader
... or from society as a whole?
4. They get a new identity based on the group
... congratulations, "Doctor": you're a doctor now!
5. They are subject to entrapment (isolation from friends, relatives, and the mainstream culture) and their access to information is severely controlled.
... and during your residency you will unfortunately have to work 80-hour weeks. This will make you miserable and leave you with little free time, but you can't leave, as you now owe half a million dollars on your student loans. Have a nice day.
I may not have gotten the mapping particularly correct, but I think that these five steps could easily describe premed, med school, and residency, too. At each step of the process, people are weeded out, thus ensuring that the people passing through the pipeline will share a common subset of characteristics. And the people who come out at the end of this process... view the world through a peculiar cultural lens. In the end, how could they *not* do so?
In short, I believe that the very training that made you a doctor actually leaves you ill equipped to address the fundamental structural flaws in your profession, because you've been carefully programmed to contextualize those flaws in a particular way.
And I don't single doctors out for this... I believe more or less the exact same thing about software engineers... which happens to be my field... though the training process is considerably different and the cultural programming steps don't fit quite as well when viewed explicitly, the end product is roughly the same: a large population of practitioners who have great difficulty seeing past their own cultural assumptions. Which is why a lot of software seems quite awful these days.
And this, finally, I think is very relevant to The Oil Drum... because I've seen all sorts of articles about the psychology of people's reaction or non-reaction to the problem of peak oil. And even "peak oil" culture itself appears to have its own peculiar cultural lens.
Hmm, the same underlying problem in several very different fields?
Perhaps humanity's fundamental underlying problem isn't actually bad doctors, a mismanaged medical industry, crappy software, peak oil, or resource depletion... perhaps it is an underlying inability to accurately perceive and act on our own problems so that we can find good solutions to ensure our long term survival?
I know you may have already written me off as a crazy person, Doctor, and fair enough; you're certainly not the first Doctor to have done so. But please don't mistake my surface anger for my desire to understand *deeply* the underlying problems that caused that anger, so that perhaps someday others won't have to suffer as needlessly as I have.
I have one I would like to suggest. Many of the problems originate from the fact that the general public has lost faith in healthcare professionals in general. Right or wrong, it would be beneficial for all those in the industry to recognize that practices by the major pharmaceutical companies and their cozy relationships with the FDA have created an environment where your patients no longer trust your motives.
The health care industry should support a tax on all drugs, the benefits of which would go to support research into alternative medicines. It isn't that there are no interesting lines of research into things like IV vitamin-C as cures, it is simply that there is no financial incentive to do all the unproductive work and explore all the blind alleys necessary to come up with interesting results. When there is no proponent for the natural remedies that can not be patented, they are simply ignored. Or if they are investigated, the clinical trials lack the vigor and enthusiasm which are applied to trials of major pharmaceutical medicines.
As the public, we want to see mainstream healthcare professionals stand up to the drug companies and the FDA. Force them to start looking into and funding alternatives lines of research that are not in their financial best interest. Because if I see a treatment option that nobody is getting obscenely wealthy from, I will have a tendency to trust it. When I see announcements like this coming from the FDA, I simply lose all respect for the profession. Meanwhile, doctors in Canada seeing great success with the treatment are simply laughing at those irresponsible Americans.
To all serious healthcare professionals, take control of your industry and stand up to the FDA and the drug companies. Don't let them kill your profession because of their insatiable greed. Trust from those you have pledged an oath to serve is the only true measure of your success, and you have lost that to a large extent because of your unwillingness to root out the corruption within your own ranks.
I think it's pretty clear that health care does not equal health. While I'm not a big fan of Western doctors and consider hospitals to be dangerous places best avoided, I don't blame the medical industry quite as much Sarah above, mostly because I think Americans have abdicated responsibility for their own health. We want a magic pill (or a magic surgery) that will counteract our bad diet, our lack of exercise, and our toxic environment without any effort on our part. When the doctor (who might mention diet and exercise as so much white noise) prescribes the pill, (along with a couple others to take care of side effects and the side effects of the side effect drugs) we take it rather than take responsibility for our lives and our choices. We create our own health. No one can give it to us.
What you said! "We create our own health".
It's often hard to be mindful in the heat of things, but it takes two to tango, and in all the painful scenes of my life, I got to admit I played along with the game(s).
I look at peak oil .... as an opportunity-crisis for people to explore deep issues of philosophy and spirituality, like:
* what is the meaning/purpose of life?
* who are we really (an epiphenomena of chemistry, or a soul incarnate in a particular bio-vehicle, or ?)
* what exactly is free will, and what are its limits?
* what about psi, reincarnation, real heavy duty metaphysics/magic?
It's so hard sometimes to really get outside of the superstitious-materialistic group-think and look at bigger issues and look in new & different ways, and then act and create the life we want.
We're faced with false choices from two dominant adolescent cliques:
Got to bahleeev in Geeezuuus or you're going to hell -vs- genetically engineered plants and nukes will save the day and infinite growth forever can continue.
(My take is both those cliques are wrong - "a plague o' both your houses")
Thanks to Rockclimber for his post.
For those who have read some of my posts on health issues you'll know that I am a big believer in large doses of vitamin C and now (partly thanks to westexas) vitamin d. How did I get this way? My mom also had health issues when I was in high school in the form of high blood pressure and high cholesterol. My mom was an avid reader of a couple of books by Adelle Davis and did achieve some sort of success with some of her issues through the use of diet IIRC. I think my older sister was in on the Adelle Davis trip for a while too and now she has evolved into a full fledged organic/health food person. My dad was diagnosed with a condition called pernicious anemia in the early nineties and his treatment with periodic injections of vitamin b12 has worked very well for the most part. When my younger sister had a bout with cancer ten years ago I started to pay some more attention to health issues but, she recovered after her lumpectomy and associated treatments so I forgot about it for a while. My mom died a couple years later from complications after having a hysterectomy which was deemed necessary after she was diagnosed with cancer of the womb. The autopsy described the condition as total organ failure, something that apparently sometimes happens to patients after an operation. She had also had hip replacement surgery necessitated by a hip fracture less than ten months before her hysterectomy and in fact, it was while she was hospitalized for the hip surgery that the first investigation into her cancer started. My younger sister's cancer returned a few years later and she died after a 18 month battle. She had discovered a lump on her neck which turned out to be some cancer in the lymph system(lymphoma?) which metastasized and spread to her spine, brain, lungs and liver. So, the death of two people near and dear to me really got me interested in how we get sick and how we get better. In my quest for knowledge I have uncovered some interesting ideas.
One IMHO, is that there was a sort of golden age of medicine in the first half of the 20th century when a lot of vitamins were "discovered". During this age some amount of persistent degenerative conditions were associated with vitamin deficiencies and a lot of needless suffering has been prevented just through the use of vitamins. AFAICT at the same time a lot of advances were being made in the pharmaceutical industry that resulted in a lot of new prescription drugs and now prescription drugs have become the de facto tool used in modern medicine. Very rarely does a modern doctor ask or care too much about the environmental factors. Rock Climber's article suggest that his opinion may be shared by the wider medical community, that they are powerless to affect the outside factors. It is far quicker and easier for doctors to write a prescription than to really investigate what environmental factors may be causing a condition. A simple example could be a bad bed causing lower back pains, a condition I experienced first hand.
Medical care has been co-opted by the pharmaceutical industry. Doctors have by and large become drug industry pimps pushing pescription drugs. One symptom of this is the abuse/overuse of antibiotics. IMHO the body has a near perfect mechanism for dealing with infections. It is called the immune system. As to why it is not perfect was explored by Irwin Stone in his 1972 book The Healing Factor: Vitamin C Against Disease reproduced on-line at the link with the permission of his estate. This kind of thinking is heretical in the Health care industry, God forbid that we should ever be able to get better without the help of prescription drugs/antibiotics(especially patented ones). I have got some insight into this from reading "The Cancer Industry" a book by Ralph Moss, a former employee in charge of PR at The Memorial Sloan Kettering Institute. One issue that I found particularly puzzling was the treatment of a substance called Laetrile by the FDA. It was demonized as being toxic due to cyanide being part of it's chemical composition although when pressed it is very difficult to come up with any verifiable cases of lethal toxicity. An interesting but possibly controversial view of this matter can be read here: The Laetrile/B17 Cover-up
I have found most doctors get very defensive when you start to discuss vitamin supplements and are quick to warn that one must be care full noyt to overdose yet far more people die from taking prescription drugs even when taken correctly than have ever died from taking a n "overdose" of vitamin supplements. Is this defensiveness because this reveals a chink in their armor?
Watching CNN one morning during flu season some time ago, the news anchor beaks into a story that went something like this "A recent study by medical researchers found that vitamin c is not effective in the treatment of colds and flu. Individuals are advised to get their flu shots and avoid contact with people with the symptoms of flu". That's it.... end of story...moves on to the next headline. I wish I had recorded it. There was no indication of who, where, when or how the study was done. Just a statement of fact and a recommendation, marketing and PR for flu virus manufacturers under the guise of news. It incenses me because from personal experience, I know that is a LIE.
Vitamin D has been making some headlines because of the mounting evidence of the beneficial effects of adequacy sun exposure on the general health and well being of human beings but, not really in the MSM since, I suppose, there is no profit in promoting free sunshine. I firmly believe that any advances in health care that do not involve healthy profits for pharmaceutical companies will be suppressed by the MSM and that doctors are just helpless pawns in that chess game. I only blame doctors for not questioning more of the "conventional wisdom" but, maybe if I had been more interested in becoming a doctor and gone through medical school, I would have been brainwashed enough to toe th party line myself. I just can not help but admire doctors like Cedric F. Garland DrPH FACE and Michael F. Hollick, MD, PhD., who have done lots of research on the health benefits of (free) sunshine. Thanks again to westexas for linking this video of Dr. Hollick making a presentation at a Diagnosis & Treatment of Vitamin D Deficiency Seminar, held by UCSD School of Medicine and GrassrootsHealth. I invite all the doctors who have responded to this article to convince me that there is some ulterior(profit) motive for these men, promoting ideas that will certainly be difficult for anybody to profit from.
The long and short of it is that the Health Care Industry in the US has become overwhelmed by greed and excess. The USA is a great country and has fostered many remark achievements but it is also home to some of the greatest inequities. Corporate greed has trumped the public interest in at least the areas of Health Care, Finance and Energy(Oil) that leads me to beleive that the love of money is indeed the root of evil. It makes me sick ;>D
Alan from the islands
I generally agree with the message of this post.
The average life expectancy in England and France was about 32 years in 1700, with two thirds of the children in London dying before their 16th birthday. This was attributed to hunger and malnutrition (weakened immune system) and to infectious disease.
http://www.amazon.com/Escape-Hunger-Premature-Death-1700-2100/dp/0521808...
The living conditions and lack of sanitation of the factory workers in industrial England were horrible beyond our imagination:
http://www.fordham.edu/halsall/mod/1844engels.html
The germ theory of disease was not proven until the mid to late 1800’s (Pasteur and later Koch).
The use of chlorine to treat municipal water in the early 1900’s led to dramatic declines in the death rates form water borne diseases. Tuberculosis, another major killer, was greatly reduced by antibiotics. Smallpox was eradicated and diphtheria, Pertussis (whooping cough), polio and other diseases were greatly reduced by vaccines.
All that being said, my own life was extended many years by gall bladder surgery , my bile duct having been blocked by sludge from gall stones, resulting in pancreatitis, which almost killed me. The pancreatitis was discovered by an MRI and I underwent laparoscopic surgery after which I was walking around 24 hours later. Eight years later I am still healthy, bicycling 10 miles at a time a couple of days a week, doing yard work, lifting weights and building houses for Habitat for Humanity. By life expectancy tables I should be around at least another 20-25 years.
Oh really? So when I got strep throat and couldn't fight it off, somehow the antibiotics that did fight it off weren't actually necessary? Or the antibiotics to get rid of a uninary tract infection. Gees, I hate to admit it but I'd be long gone in this life without medical assistance.
"...once a certain point of basic knowledge and practice is reached" should certainly be an addendum. If, for example, smallpox were still endemic and we lacked the basic knowledge of what it was or how it was transmitted, then our lifespans would surely be shorter on average.
I've been very healthy myself, but 15 years ago I did get double pneumonia and was treated with antibiotics, but that was commonly fatal in the old days without medical care.
The key word in your quote is AVERAGE. It was serendipitous for you that the antibiotic therapy was successful. The millions of 'you's in the same situation contributed to the 2% increase in 'average' lifespan.
Al
Man Adapting by Rene Dubos is a good book that deals with this larger picture of health of individuals in a society and the world at large.
How much of the increased average life expectancy in the top countries can be atributed to superior law enforcement and lower birth rates?
Rock Climber writes:
The chain of causality is not quite as simple as that. The independent variable is not poverty as such, but cognitive ability or information processing capacity. People with low IQs tend to get poorly paid jobs (on average) or to be unemployed / unemployable. Because the poor are less educated and less educable, they also tend to be less well informed and thus less concerned about the adverse health effects of smoking, alcoholism, and overeating.
Poverty inside rich countries, in other words, correlates with poor health. It may be a proximate cause insofar as poor people's low social status makes them more prone to addiction as an escape from the frustrations of their everyday lives. But the ultimate cause is that people are poor because they are cognitively disadvantaged. And because they are cognitively disadvantaged, the 'just don't get' when it comes to understanding the importance of a healthy lifestyle as a determinant of longevity and, well, of good health in general.
I think you are assuming that the societal/economic system does an efficient job of sorting by ability. I don't think the sorting is nearly so efficient. Clearly on average the lower classes are lower in ability. But, many highly capable people fall through the cracks. Perhaps there skills just don't match up with job openings, or they interview poorly, or have some minor psychological hangup that causes opportunities and them to not connect. And we have the converse, people of little apparent ability rising to great wealth. I really wonder about the mythical 1% in the USA. Few honourable professions provide that level of income, and then only to a tiny minority among them. And it seems that many got there by exploiting things that I had thought of myself, but considered to be unethical.
But in any case, we have a class/economic system where intelligence/ability improves the odds of a good outcome, but does not guarantee it.
Rock Climber writes:
Hmmm ... sounds as though the Cornucopians, under the banner of St Julian Simon and Blessed Bjorn Lomborg, are at the gates of TOD.
Time for Rock Climber to do some further reading:
http://www.garretthardinsociety.org/
This is a brilliant post by a brilliant doctor. IMO it is the best post I have ever read on TOD. It is obvious that he put a lot of work and thought into it. I can find nothing to pick on except I think he is overly modest about doctors saving lives.
Doctors have saved my life at least 3 times. It appears the doctor is counting a life saved as one per person. In my case and no doubt in many other cases, doctors save one person multiple times.
As a boy I fell and broke my arm. Seems minor but I might have died or been maimed for life had a doctor not set it and put it in a cast.
In 1964 as a draftee in basic training I slipped on the overhead bars and fell breaking my left elbow. Army doctors operated, put in a stainless steel screw and set it, then promptly lost by medical records.
But they saved my life for sure not so much by fixing my broken elbow but by getting me separated from my unit which was mostly sent to Viet Nam. I was later sent to much safer Germany.
In the early '70's I could have been killed in a car crash at a rural intersection when another car hit me on the driver's side door. My knee was sore for weeks. I did not see a doctor, but clearly could have been killed if the crash has happened at a higher speed.
I didn't see a doctor again for many years until 1999 when I noticed by feet were numb. My sister had purchased a blood glucose meter and my blood sugar tested 300. I went to the doctor who found that my A1c tested 13. I count this as the second time doctors saved my life.
One year later after losing a lot of weight and drinking a lot of diet drinks (aspartame) I had a sharp pain in my right side. I went to the doctor who ordered a CT scan which found a renal cell carcinoma
tumor about the size of a quarter in my left kidney.
I had a nephrectomy of my left kidney. This is the third time doctors saved my life.
Since being diagnosed diabetic, I am one of the "frequent fliers" as the doctor points out in his post. But with out intervention of doctors I would have died at least 3 times.
I am being treated for hypertension and high cholesterol too. So it may be that doctors have saved my life up to 5 times so far.
In longevity statistics you only die once. But in the real world people face death multiple times and survive, but statistics ignore it except for a small blip in life expectancy which is averaged out with all the other medical successes/failures and societal failures as the article points out.
These multiple life savings are undervalued in the statistics but are highly valued by the beneficiaries.
Quality and Quantity of Life from TOD and bicycling
People that bicycle to work live 10 years longer than those that do not. +12 for improved health, -2 for accidents. Increased bicycling keeps the overall fatalities steady or reduces the #. So the rate drops dramatically and x10 the bicycling will bankrupt Social Security because of increased life span.
Walking also does a lot of good for health, especially if it is part of a lifestyle and is done several times/day instead of "going to the gym". Depending on Urban rail just naturally creates walkable neighborhoods over time.
Best Hopes,
Alan
Alan,
If the bulk of society switched to electric rail and bikes air quality would improve. See Atlanta 1996 in the olympics, pediatric asthma admits dropped by a huge margin.
-matt
HI Alan,
I'm glad to hear some positive news! in a currently less-than-positive-on-the-immediate-front chain of events.
Although I've noticed lately that on bike, I have a near-collision experience approximately every 10 days - cyclists without lights, mostly.
Then, a couple of weeks ago, in an effort to bypass the least safe portion of the bike path at night, I took a detour, and ended up spilled out, though on grass, luckily enough.
I'd like to go back to handing out free lights, if I could get the funding.
Stress will kill you. I never went to a doctor until fifteen years ago. My son was killed in a car accident and the stress almost killed me. After that my health went down hill. Kidney stones, gout, high blood pressure, diabetes, back problems, allergies, gallstones, and cancer are things I recall off the top of my head that I developed. I went from a very healthy man to a person who is disabled in a few short years. Stress will kill you even if your not a baboon.
hotrod
This is sort of a I wore blue socks and won the big game argument. I am not saying stress is not contributory but we all die someday. You getting a host of age related illnesses that develop over decades is coincidental with preceding events. Hope you can get out of the house and feel better.
There's a large body of scientific evidence about the very real connection between stress and disease. Check out Gabor Mate's work:
http://www.amazon.com/When-Body-Says-Understanding-Stress-Disease/dp/047...
I read somewhere, I don't remember where that vitamin C is used in the production of stress hormones. As a result sustained high stress conditions will reduce circulating levels of vitamin C to levels that severely impair immune system function and leave the body vulnerable to all sorts of opportunistic infections. Sounds logical to me! I figure that this is one of maybe many physiological factors that link stress to ill health.
Alan from the islands
lineman,
"IMPORTANT DISCLAIMER: POPULATION HEALTH IS not individual health."
Overall, this post resonates very strongly for me, having grown up in a family with a doctor dad and nurse mom, nearly going into medicine myself, and now deeply engaged in trying to connect the dots for people who generally do not compute (especially in the realm of environmental, social, and human health, politics, energy issues and climate change). But I was just lurking here until I read your comment.
Per the disclaimer, the post is about population health. And yet as a fellow human, wired to respond to individual, not population, stories first and foremost, I must stop to say how sorry I am about your son and your loss. Though I do not know you, I know how profound and personally damaging such a loss must be. Your words, brief as they may be, speak volumes.
Please do not give up. Seek some sort of therapy - holistic or spiritual may be most helpful. You can likely still recover some of your health.
I too suffered an unexpected and horrific loss, though it was a close friend who was killed in an accident, not a blood relative. In the past many months, my health has declined markedly, but I kept telling myself that after a year, it should be time to get better. It didn't help. Finally, I went to seek treatment for seemingly unrelated but potentially disabling physical symptoms. After several weeks of treatment, the practitioner said that the peripheral problems kept signaling back to a deeper heart/lung problem, and that was most often linked to profound loss. I had up until that point mentioned nothing about my friend's death. Once I confessed, the therapist nodded sympathetically, and said we had more work to do. I am not a touchy-feely woo-woo kind of person, but suspending disbelief and using the power of social support - perhaps the placebo effect - is proving extremely healing. It also has avoided extensive and expensive high-tech diagnostic testing.
Good luck. I hope you can recover at least some of your health. Dying of a broken heart is not a metaphor, alas.
Wow, quite a discussion here. That was an excellent article posted by Rock Climber and I am in substantial agreement. I have long believed that our health is mostly determined by external factors as opposed to what our health care system dictates, provides, etc. It is primarily a result of our own actions or lack of actions throughout our lives, many of which our society collectively decides are best and are served up as "cultural norms." Our natural tendency is to go along with these cultural norms even if scientific realities may point us in a different direction. Given this fact, I do question what percentage of our decisions can actually be attributed to not understanding the "dark matter." I would argue that many people are aware of at least some of this dark matter but still do not act on it because it is not congruent with their long held cultural norms and beliefs.
When people are confronted with scientific realities that may be different from established cultural frameworks this often causes cognititve dissonance. Once this happens we usually ignore the science and go with cultural norms even to our detriment. If you point out these conflicting scientific realities to people they will either ignore you, think you are crazy or forget about what you said. Anyone who has tried to explain peak oil to people knows exactly what I mean. This type of behavior has been going on throughout history. I believe it is why so many people are ignoring: peak oil and other resource depletion, our reliance on excessive debt, our need to change a broken health care system, to redesign our communities, etc., etc.
Ecological economist, William Rees, from UBC has recommended several books on this subject including:
-Don't think of an Elephant by George Lakeoff;
-Brain and Culture: Neurobiology, Ideology, and Social Change by Bruce Wexler;
-The Crowd: A Study of the Popular Mind by Gustav Le Bon
I am also a fan of Sapolsky and have enjoyed reading his books "Why Zebra's Don't Get Ulsers" and "Monkeyluv : And Other Essays on Our Lives as Animals." In addition to being a brilliant neurobiologist he is a hoot.
I liked very much the article.
Speaking about medical dark matter, I believe that in human health there is an energetic component. I am talking about a kind of energy unknown to conventional medecine, vital energy or something like that. I am a practitioner of energetic therapies in Spain, and I wouldn't say that those kind of therapies can cure cancer, parkinson or alzheimer, but, if you are lucky enough to find a professional that actually knows what he is doing, they can cure your backache, headache or many functional troubles in +/- 80% of the cases. As we have read here that stress is one of the main causes that reduces lifespan, and it is clear that having headache for 30+ years should stress you, how can those therapies not contribute to prolong your life?
As always, not everything is true in complementary and energetic therapies, but also not everything is true in conventional western medecine.
I speak about vital energy being the dark matter because, at least in my country, what conventional medical doctors can do for your cronic musculoesqueletal pain is to give you analgesics and anti-inflammatories, that probably are good for acute problems but don't cure cronic cases, and certainly should not be ingested for years on end.
TOD is a cultural treasure. Great articles like this one and so many more here.
Regarding the medical 'dark matter'. I recently came across some web sites discussing sit vs squat toilets and potential health effects of the former. I have seen many studies comparing diet, but had never even considered the possibility that the 'sit' toilet could lead to health problems by itself. Perhaps this could account for a little of 'dark matter' affecting so many.
OMG!
I recall reading an article about that when I was in nursing school (back in the dark ages) They specifically linked population hip joint health and flexibility to the use of 'squatting' facilities. Since reading that I have squatted daily. My hips are fine, TYVM. Funny to find mention of this in TOD. LOL
Al
I think Sit vs. Squat toilets also have an effect on the spreading of germs, in that with Squat, you don't touch anything. You do need a certain level of fitness to use them, however.
Fantastic article, with really well presented data. Rock Climber actually does a great job invalidating his own metaphor. "Dark matter" and "dark energy" are terms physicists use to mean they haven't got a clue as to why some observations don't support some of their theories. No one has actually found "dark matter" or "dark energy". However, RC has found and listed the most important factors affecting longevity - and they are not what most people in this country would think. Thanks for posting this Nate.
Thank you for a very fine article, Rock Climber.
Some great discussion in comments also.
Rock Climber -- I live in the Central neighborhood of Minneapolis -- maybe 10 blocks south of Abbott Northwestern Hospital.
If you are in the Twin Cities or nearby, it would be great to have coffee. I can show you my Organic Engines Sensible Utility Vehicle, talk EV's, Peak Oil, or related topics.
My guess is that I will be in the heart of the city here for at least a few more years -- maybe more.
At any rate, thanks again. Feel free to contact me at
gmghoover (at) comcast (dot) net
My mother died when I was four. With four siblings, and an alcoholic native american father, we were all placed in foster homes. I personally had 14 different families that I lived with growing up. I'm 57 years young now. My youner brother died in Germany while in the army. My middle older sister died too early at the age ofg 52 from cancer that spread rapidly through her body. I have been blessed with a healthy family, two children, and a wonderful wife.
I'm a social gerontologist who develops and operates assisted living centers....currently with 270 residents in various communities of care...as I call them. I employ about 180 people, hearts and minds I tend to refer them as. Building communities of care is rewarding. We see the "health care system" generally improving regarding end of life issues, and "futile medicine", as it's called. Hospice has been a key player in this evolution, bringing acceptance and a saner view to the process of end of life. Blessing to hospice workers everywhere.
A good book....The Denial of Death...The Denial of Death is a work of psychology and philosophy written by Ernest Becker and published in 1973. It was awarded the Pulitzer prize for general non-fiction in 1974. THere is much in our culture that is f***** up regarding the issues of health, happiness, death and dying. That said, we continue to evolve. I see it.
I see my work as sacred....caring for people at the end of their lives. In general, it seems that those who have lived a life of general happiness, kindness and amiability get more like that as they age. Those whom are contentious, negative, meanspirited and gernally curmudeons, tend to be more like that in their old age.
My internship took me into ResQuip committees where hospital higherups decided how to cover up mistakes. I've recently heard that there are 98,000 iatrogenic deaths annually in the U.S. When I or one of my family get sick, there is a wealth of diverse sources of treatments. We're fortunate to live in Colorado, where Boulder is nearby, with many alternative treatments that range from very intelligent offshoots of the MD world (that deliver an amazing combination of medicine, treatments, counseling, herbology, diet alternates, etc.) and we've never had a difficult time finding wellness.
Once, having fallen through a reinforced glass ceiling and severly severing my ulnar nerve, I underwent about two hours of surgery at 3 in the morning. Some wonderfully trained surgeon got out of bed to save my hand. I've since given up a lot of bar chords, but like Woody Guthrie said, "If you need more than three chords, you're just showing off."
A dear friend who suffers greatly from PTSD is on way too many medications, which I plan on looking into for him. A few years ao he was homeless in SanDiego. A friend from the 60's found him and put him in charge of watching over a small ranch in the Rockies.
Life is amazing to me. I spent a decade in the 70's traveling the world and meeting wth many leaders of ashrams, cultists, shamans, monks, etc. The answer was found when I took a year long retreat into deep wilderness.
The answer? Relax. Stress is the leading cause of all our illnesses. Anyone want to do a campfire discussion on stress and how to mitigate it?
Nate,
It seems your friend is struggling to find an answer as to why US medical care has deteriorated so badly over the years, despite increasing amounts of money spent on health care, when the answer is quite apparent within his own argument (loosely quoted).
”Despite over $2 trillion a year of modern medical care, US life expectancy has dropped to 50th in the world behind all of Europe and behind some very poor countries. It seems to me that societal factors account for about 85% of differences in life expectancy. Social factors- differences in our artificially created everyday living conditions- are the real keys to human health. Health is improved by money, social status, healthy early childhood, education and a good job. Poverty and lack of control hurt health. Money buys health for individual rich Americans, but has failed to make average Americans healthier. What we decide about health care reform will have no effect on US life expectancy, since doctors have so little influence on health. Like everything else in our artificial modern world, health care and energy problems are really economic and social policy issues.
SIMPLE INCOME IS THE BIGGEST DETERMINANT OF "AVERAGE" LIFE EXPECTANCY (my capitalization for emphasis).
US inequality worsened in the past 30 years. In 2008 the top 10% of the US population got 48.5% of total income, the top 1% got 23%, and just the top 1/100 of 1% (14,988 families) took 6% of it all."
He states, but cannot seem to face the truth, that the problem is the US medical establishment itself, including doctors, hospitals, insurance companies, pharmaceutical manufacturers, and those "investors" who benefit quite handsomely from the ill health and sickness of others.
The mistake in his key argument that, "average" life expectancy will not be improved is misleading because using a "simple average" results in his drawing a wrong conclusion, something simple averages are prone to do. The question cannot be adequately answered by using simple analysis. He could start by using a "weighted average" to "follow the money." Assuming that money spent on healthcare yields benefits to someone, if the US is spending increasing amounts of money, yet not seemingly attaining the desired results, then where is the money going and who is it really benefiting? From that point, the answer should be relatively simple to determine.
What he is arguing quite strongly for, but cannot seem to grasp the concept, is socialized medicine similar to that commonly found in most "civilized" countries. The US has some of the worst medical care by design, primarily because it is designed to provide profits for the wealthy, not provide cures for the sick.
That, however, won't completely fix the underlying problem of the increasing disparity of income between the wealthy and everyone else, but it would at least be a reasonable start.
I strongly disagree that health care reform (not Obama-style health care reform) will have no effect on US life expectancy, which is borne out by the statistics from health care programs in other countries where it is designed to actually provide health care, not wealthy-care.
What is truly egregious is to have an argument like this made by a person who has taken the Hippocratic oath not harm his patients. His argument, that spending more money on health care will not prolong life, is just what the wealthy medical establishment wants to hear from supposed health care professionals in order to avoid having to provide decent health care at a reasonable cost.
Gordon 2342
There is a lot of truth in this statement....and don't forget the corporations who heavily market unhealthy fast food to our population. An excellent discussion of how the US stacks up against other countries in terms of health care expenditures in some of these categories is contained in T.R. Reid's book "The Healing of America."
As RC pointed out, despite their much lower expenditure for healthcare as a % of GDP, life expectancies are higher in most of the other major developed countries. Although, I still believe that the cultural norms of walking, biking, eating healthy food, the way they land planned their communities and transport systems, etc. (designing for and living healthy active lifestyles) in these countries are by far the most important factors in achieving long term good health. This is also why it is going to take longer for the US to reverse its negative trends and make this transition, that is, if we don't run out of time and money first.
"When we resist our fate we suffer.
When we accept it we are happy."
???
I'd like to put in a link I got from TAE.
http://www.wired.com/techbiz/people/magazine/16-01/st_thompson
This refers to an academic who coined the term Solastalgia to describe the mental illness you get when you feel homesick when you're at home.
Perhaps not surprisingly, he found these people in an area ripped apart by strip mining of coal - what we call in the UK opencast.
Previous generations of humans could up sticks and find somewhere new. Not the same now, when your garden becomes a dustbowl and the hills go flat.
You stay in the only house you possess. And become ill.
Gosh, I am really shocked how bloody minded a few of the people on this thread are. I shall not name names, but if the shoe fits. . .
I realize that the present global population is probably unsustainable and must inevitably come down, one way or another. I rather suspect it will do so due to a large number of small catastrophes rather than a single massive one. I really must totally disassociate myself, though, from this advocacy that medical care should be cut back or even totally eliminated in order to hasten and intensify the die-off.
First, I must point out that while population overshoot is a global problem, we don't have a global government. What we do have is a couple hundred national governments. It is each nation which must cope with its own population problem and its consequences.
Second, I must point out that the human population is not distributed evenly over the Earth's land surface. Some nations have far higher population densities, and are much farther into overshoot, than others. To the extent that there are inevitable reductions in human populations in the future, these reductions are going to be uneven as well.
My particular interest, and the primary focus of the article at the top of this thread, is the North American context. I must note that population densities for North America are considerably lower than they are for places like Europe and East and South Asia. While I am not really comfortable with a US population of 300 million (and am very nervous about it increasing to 450 million by mid-century), it is nevertheless true that we have plenty of land and water that could be put to productive use, and that we can most certainly feed our population, even without continued inputs of FF energy and petrochemical fertilizers and pesticides. I just fail to see any good reason why a massive population die-off in North America should happen or needs to happen. I certainly don't see any good reason why such a die-off should be promoted or enhanced by such things as shutting down the entire medical care system.
Let's get real here: A snowball in hell has a better chance than does any serious policy proposal to shut down or radically curtail the medical care system in the US. That just isn't going to happen, and everyone here should know that.
Of course, there is always room for voluntary action. If there are those who believe that medical interventions only keep alive those who need to die, and the sooner the better, then what keeps them from refusing to seek treatment for themselves? It would seem to me that anyone who has posted suggestions to the effect that medical care should be curtailed in order to increase mortality rates need to be the very first to volunteer, if they are to avoid having the label "hypocrite" applied to them.
Now it would not surprise me at this point for someone to launch into a tirade about overpopulation. For your information, I have drawn a "Get out of the population lecture for free" card. My wife and I did not have children, and we are much too old to attempt it now. Thus, while I recognize that overpopulation is a real problem, it really isn't MY problem. I didn't contribute to it, and it will not be my offspring that will suffer the consequences. It would thus seem to me that those of you who have had children should have nothing to say to me about population at all.
Since a lot of other people have put in their 2 cents (and sometimes a dollar), I'll add my random thoughts to this very good discussion.
Having tried to become a BTO (big time operator) and failed in farming, we as a family are struggling to find our way, hanging onto the family farm, using off-farm jobs, renting out most of our cropland and retaining pasture for our cattle herd, which is making the mortgage payments. We can't afford health insurance and have been rejected for Healthwave (state-run coverage) for our kids for two years, as the clerics in Topeka don't know how to read business tax returns (they tend to equate gross income with net, and assume we have "all" that income to spend as we see fit. We have bought individual policies for our kids as money has become available.
My Dad had a massive heart attack in 1981, followed by a 4-way bypass that saved his life. I credit the quick thinking of a lady who happened to be sitting beside him in church who recognized the symptoms and drove him to the hospital before his attack actually hit. I credit the hospital staff and surgeons who handled the trauma very well. However, his attack stuck him with his insurance company, which proceeded to raise his premiums until he had paid all the medical expenses back plus a healthy (unhealthy?) profit before he was old enough for Medicare. After three more attacks,starting in 1997, he finally succumbed in 2004 while walking to the pasture to check on the cows, when the third one hit him. Each time, the experts sent him home to die, but he was back on a tractor in a month. Mom actually blames his death on the drugs he allowed his doctor to prescribe, Paxel in particular.
The health advice given to him by the "experts" would have killed him way back in the '80's had he followed it. Even though I was striving to be a BTO, I was having big doubts about the whole system and was looking at alternatives then, so I could give my Dad choices. Since my college major was animal science, I tapped into that knowledge and realized human nutrition was atrociously behind. The diet they tried to put Dad on (bland, no salt) I knew from empirical studies on pigs would kill him. Mom and I put him on fresh food, largely home-grown, vitamins (good ones, not from large corporations) and minerals, plus exercise. (With modern agriculture, farmers are notoriously out of shape.) He got plenty of farm-fresh eggs and home-grown beef and lamb, fed without antibiotics and all the other hormones and junk the experts recommend, and real butter, not margerine. When he died at 76, the mortician was amazed at his muscle tone. He'd never prepared a body that old that was so strong, rivalling men in their 20's.
I feed a natural product to our livestock and eat it myself. It's a menefee humate from New Mexico, recommended to me by a friend involved in natural fertilizers (been using it for 15+ years). It contains a primitive bacteria that goes into spore form when conditions are bad and back to a bacteria when conditions are good. It digests the woody tissue of plant cell walls, making about 30% more of plant matter and minerals available. It also contains trace minerals, and the carbon appears to have special properties that absorb toxins produced by biological diseases, thus helping natural immunity to stay strong. It works so well, the only time I need to vaccinate is before I sell my calves, largely to satisfy the "system". The cost is minimal--less than $.03/head/day.
The balance of minerals in the soil is extremely important. I recommend the writings of Dr. William Albrecht, former head of the Agronomy Department of The University of Missouri, before Monsanto started pumping research money into it. I also recommend Neal Kinsey (www.kinseyag.com) for soil improvement. My experience tells me that farm animals can get by in a tough winter or drought if they have a good supply of minerals. Dr. Albrecht's research led him to the conclusion that animals eat short-term for taste, but long-term for minerals. Transfering that to human behavior, is it possible that our obesity is a result of our craving for minerals not present in our diets, causing us to eat more and more, especially sweets and starches and even mood-altering drugs? In the wild, plants that have a good mineral content are also sweet. Is modern food manufacturing, perhaps unknowingly, taking advantage of that built-in behavior to sell us crap? Toward the end of his life, Dr. Albrecht made the outrageous statement of "Tell me where you got your cancer and I'll tell you what minerals you've been deficient in for years", since different organs vary in their mineral needs. In my area of the high plains, our soil is horribly lacking in selenium and copper. Selenium is directly tied to prostate health and (surprise, surprise) men around here have a high rate of prostate problems. Some of the health problems were alleviated when we shipped food around, thus mimicking the buffalo's migration north and south on these prairies, picking up various minerals and storing them in their marrow, but with the modern emphasis on yield, coupled with DNA manipulation, and soil degradation, we can grow food that looks good and tastes sweet (modern carrots,for example) but lack minerals. I suggest getting a good refractometer and learn how to use it to monitor your own gardening/farming endeavors.
My wife works at the local nursing home, an excellent facility, and they are feeling the pinch of actual cutbacks in state Medicare. Hours are reduced, and other cost-cutting measures are being implemented, much to the chagrin of the half of the residents who can afford to pay their own way. ("For $4000/month I'm paying, you are not going to turn down my thermostat when I'm not in my room!")
Part of the problem of a complex society is that we become so specialized, few of us have the ability to step back, look at the big picture, and say the emperor has no clothes. A BIG share of our GDP is money spent to alleviate the problems caused by not thinking long-term about new ideas, products and processes. Subtract the money spent on fixing the problems (health care, pollution cleansing, etc.) and it quickly becomes apparent we have little or no real wealth. In the nursing home, for example, a lot of effort is spent adding drugs to counterbalance the detrimental effects of the previous drug that was prescribed to alleviate the effects of the previous drug, and so on.
Thank you all for the many excellent responses to the “Medical Dark Matter” paper.
I agree with the many posters who emphasize clean water, vaccines (yes I believe they work great, although the recent H1N1 experience has revealed ways public health doctors have over sometimes oversold the horrors of vaccine preventable diseases and the safety and efficacy of vaccines), maternal health, appropriate antibiotics (widely abused for viral and self limited conditions, but are true miracle drugs) and trauma care. I can’t prove that kind of very basic medical care (like I delivered for Doctors Without Borders) works, but I think it does. I can’t guarantee a healthy lifestyle will work for anyone, but I think it often does.
I could be wrong, but my best read of the available data is that whether US healthcare is broken or not, adjusting it won't much affect our longevity. If we stuck to perhaps the most basic 5% of medical care we'd lose only 2 months out of 78.1 years on average and gain $2 trillion annually. Maybe we could do a lot of good with an extra $6700 per person per year.
I think Europeans live longer not because of single payer healthcare (a more economic and just system) but because their living conditions are more health favorable than the US.
Thank you all for helping me better understand and communicate this difficult subject. I agree change will be all but impossible. Single payer makes much sense but is politically 'off the table'. Reducing futile, cruel end of life care (ICU deaths with a tube in every orifice increasingly borne disproportionately by poor people of color whose doctors can't or won't communicate well with them) would reduce human suffering, but is quickly called 'death panels'. People angrily defended the status quo in healthcare reform town hall meetings. (My favorite comment was "Keep your damn government hands off my Medicare!").
I figure TOD is ground zero for inconvenient truths. Further suggestions are appreciated.
Indeed. The appalling level of ignorance, cognitive dissonance, and schizophrenic nature of what passes for healthcare "debate" in the U.S. is breathtaking to behold for its better informed citizens. I imagine it must look truly bizarre for any inhabitant of the first world (omission of U.S. intentional).
Thank you all again for the many excellent responses to my “Medical Dark Matter” paper.
First, to Sarahannalien, I apologize for the pain my profession has caused you. I hope there is some way for you to become less reliant on the doctors you probably despise for good reasons. I agree with you on some points. Doctors can be faulted for taking a lot of money to do little and are not gods or priests. Doctors have elevated their cultural importance to the point many smart people think doctors saved their lives when in all likelihood they did not. Doctors should emphasize their oath to “first do no harm”. I know this will not go far enough for someone who is so mad (your solution is to kill all the royals?) but I will continue to give talks to my colleagues, for whatever that’s worth.
My main “discovery” is that what I was trained to do (largely giving expensive pills) has so little impact on health. Common social factors like where you live and your job have effects up to a 100X bigger than my best treatments. I believe stress from social hierarchies will probably emerge to be even bigger health factors than our poor health choices. While admitting many faults of my profession and favoring single payer (for economic and justice reasons), I don’t think restructuring our care will even begin to dent the several year health gap our nation has developed.
I realize I’m probably rather optimistic for TOD, and I look forward to telling my wife I’ve been branded a Cornucopian. Seeing a big problem my colleagues don’t(actually many honest individual doctors do, but the AMA isn’t going to invite me as keynote speaker anytime soon!) makes her think I’m a doom and gloomer.
I know history and objectivity can’t predict a novel new event, but religious fanatics and scientists who’ve thought we are living in the end times have been consistently wrong for 1000 and 200 years (respectively since the Middle Ages and Malthus). My population health research has actually made me more optimistic about most of humanity (Africa could be an exception). Economic development was good for most of humanity and probably boosted global average life span about 35 years between 1900 and 2000.
I think we may get precariously close to a disastrous die off, but I hope we’ll move away from our relatively unhealthy, violent and planet polluting ways just in time. Despite all the wars, famines, economic divides, political craziness and clueless citizenry, overall our society might be improving in my lifetime. When I was a kid in Kansas respectable churchgoing people called ‘coloreds’ (the preferred term) ‘niggers’ in public. Like him or not an African American is President now. Our children’s generation is far more liberal minded. There is no way of knowing the future with certainty. The next big crisis could be Peak Oil, Financial Meltdown, or something “out of the blue” (the New Madrid Fault? Avian Flu instead of Swine Flu? Nuclear War?). Generalized disaster preparations could turn out to be prudent, or a melancholy waste of time. You choose.
Thanks again for your helpful feedback. I remain hopeful rational inquiry will eventually help get our society back on track.
Hello, rock climber,
Thank you for your work. In case you happen to check back, I wanted to let you know about something I've mentioned from time to time that seems to me to be a positive way to do many things: emergency preparedness, "building resilient communities" and more.
An overview is here: http://www.ashland.or.us/Page.asp?NavID=541.